

Former hospital defense attorney · Law Offices of Jorge L. Flores, P.A. · Miami, Florida
Last Updated: April 2026
A Stroke Is a Race Against the Clock. Misdiagnosis Means the Clock Ran Out While the ER Was Looking Somewhere Else.
Every minute a stroke goes undiagnosed, nearly two million neurons die. That number is not rhetoric. It is the calculation published in the neurology literature, and it is the reason the entire emergency medicine system is built around speed: door to CT, door to needle, door to groin puncture. When a patient walks into a Miami emergency room with sudden weakness on one side of the body, slurred speech, or a facial droop, the standard of care demands a stroke code activation, neurological examination, and CT imaging within minutes. Not after the cardiac workup comes back negative. Not after the blood alcohol level returns. Now.
The problem is that strokes do not always announce themselves with textbook symptoms. A posterior circulation stroke can present as vertigo, nausea, and an unsteady gait, symptoms that a busy ER physician may attribute to an inner ear infection, a migraine, or intoxication. A transient ischemic attack may resolve before the patient reaches triage, leading the physician to conclude nothing happened. A young patient may be dismissed because “you are too young for a stroke.” Each of these diagnostic errors has a specific footprint in the medical record: the triage note, the differential diagnosis, the imaging that was or was not ordered, and the time stamps that document exactly how many minutes or hours passed before anyone considered that the brain was dying.
⚠ The Treatment Window Has a Hard Deadline. The Legal Window Does Too.
Florida’s statute of limitations for medical malpractice is generally two years from the date of discovery, and wrongful death claims generally run two years from the date of death, though specific deadlines can vary based on the facts and statutes in effect. The ER records, the imaging orders, and the stroke code logs must be preserved before the hospital’s retention cycle overwrites them.
The Stroke May Have Been Missed If:
✓ You went to an ER with sudden weakness, speech difficulty, vision changes, severe headache, or vertigo and were told it was a migraine, anxiety, an ear infection, or intoxication.
✓ A CT scan or MRI was delayed for hours or never ordered during your ER visit.
✓ You were not offered tPA (clot-dissolving medication) or thrombectomy despite arriving within the treatment window.
✓ A stroke was found on imaging at a later visit after the ER discharged you with the same symptoms.
✓ Your family member’s condition deteriorated in the ER while the team pursued a cardiac or psychiatric workup instead of a stroke code.
If any of these describe what happened, the ER triage notes, imaging orders, and time stamps deserve an independent review by a neurologist and an emergency medicine specialist. We arrange that review at no cost.
On This Page
TIA, Ischemic Stroke, Hemorrhagic Stroke: Why the Type Changes Everything
Where Stroke Diagnosis Goes Wrong in the ER
The Forensic Stroke Timeline: Three Windows Where Minutes Were Lost
AI Diagnostic Tools: The New Negligence Angle Most Attorneys Miss
Who Is Liable When a Stroke Is Missed
What a Missed Stroke Costs: The Injury, the Recovery, and the Life Care Plan
TIA, ISCHEMIC STROKE, HEMORRHAGIC STROKE: WHY THE TYPE CHANGES EVERYTHING
A transient ischemic attack (TIA) produces stroke symptoms that resolve within minutes to hours. The brain recovers, but a TIA is a warning that a full stroke is imminent. Studies show that up to 10 percent of TIA patients suffer a completed stroke within 90 days, with the highest risk in the first 48 hours. When a Miami ER evaluates a patient whose symptoms have resolved and discharges them without brain imaging, antiplatelet therapy, or urgent neurology follow up, the TIA that was dismissed as “resolved” becomes the missed warning for the stroke that follows.
An ischemic stroke is caused by a clot blocking blood flow to the brain. It accounts for roughly 87 percent of all strokes. Treatment is time dependent: tPA can dissolve the clot if administered within 4.5 hours of symptom onset, and mechanical thrombectomy can physically retrieve a large vessel occlusion in selected patients up to 24 hours from onset. The failure to diagnose an ischemic stroke in time to deliver either treatment is the most common basis for stroke malpractice claims in Miami-Dade County.
A hemorrhagic stroke is caused by bleeding into the brain from a ruptured vessel. It requires an entirely different protocol: blood pressure control, reversal of anticoagulation if applicable, and neurosurgical consultation. Administering tPA to a patient with an unrecognized hemorrhagic stroke can be fatal. That is why the first imaging study in any suspected stroke is a non-contrast CT to rule out bleeding before any clot-dissolving medication is considered. If the ER skipped imaging and administered tPA, or if the CT showed hemorrhage and the team did not recognize it, the type of stroke determines the theory of the case.
Anterior circulation strokes affect the carotid territory and produce the classic symptoms: facial droop, arm weakness, speech difficulty. Posterior circulation strokes affect the vertebrobasilar territory, the brainstem, and the cerebellum. They produce vertigo, double vision, gait instability, and difficulty swallowing. The distinction matters because posterior strokes are misdiagnosed at dramatically higher rates. The symptoms overlap with benign conditions, and many ER physicians default to the benign explanation without performing the examination or imaging that would distinguish them.
WHERE STROKE DIAGNOSIS GOES WRONG IN THE ER
Competitor websites list common errors. They say “failure to order imaging” and “delayed treatment.” Those phrases describe every misdiagnosis case for every condition. The failures in stroke cases are specific, and the medical record captures each one with timestamps that allow a neurologist to reconstruct exactly where the diagnostic process broke down.
The Posterior Circulation Trap: When a Stroke Looks Like Vertigo
Anterior circulation strokes produce the symptoms everyone recognizes: facial droop, arm weakness, slurred speech. The BEFAST mnemonic (Balance, Eyes, Face, Arm, Speech, Time) is designed to catch them. But posterior circulation strokes, those affecting the vertebrobasilar system, the brainstem, and the cerebellum, present differently. The patient reports room-spinning vertigo, nausea, vomiting, difficulty walking, or double vision. In a busy Miami ER, these symptoms are routinely attributed to benign positional vertigo, labyrinthitis, or a viral inner ear infection.
The clinical test that distinguishes a peripheral cause from a central (stroke) cause is the HINTS examination: Head Impulse, Nystagmus type, and Test of Skew. It takes minutes to perform. Published research shows that HINTS performed by a trained examiner is more sensitive than an initial CT for posterior stroke. If the ER physician did not perform the HINTS exam, did not document the nystagmus pattern, and attributed the vertigo to a benign cause without imaging, the failure is captured in the chart: what was documented, what was tested, and what was not.
Failure to Activate the Stroke Code or Order Timely Imaging
Every Miami hospital with a stroke program has a stroke code protocol. When it is activated, the system moves: neurology is paged, imaging is prioritized, the CT suite is cleared. When it is not activated, the patient sits in the general queue. The CT that should have been completed in 25 minutes is performed in two hours. The neurologist who should have been at the bedside within 15 minutes is never called. The tPA window, which closes at 4.5 hours from symptom onset, expires while the patient waits for imaging that was never prioritized.
The ER’s electronic medical record timestamps every order, every result, and every notification. The stroke code activation log, if it exists, shows when the code was called and who responded. If the code was never activated, the absence of that log is its own evidence. Our emergency medicine experts compare the documented timeline against the hospital’s own stroke protocol and the national benchmarks published by the American Heart Association and the American Stroke Association to determine whether the response met the standard or fell short of it.
Misread Imaging and Dismissed Radiology Alerts
A non-contrast CT of the head is often the first study ordered when stroke is considered. It is excellent at detecting hemorrhage but limited in its ability to detect early ischemic stroke, particularly in the first 6 to 12 hours. A CT angiography (CTA) or MRI with diffusion-weighted imaging is far more sensitive for identifying an acute ischemic event and localizing a large vessel occlusion that may be eligible for thrombectomy. When the ER ordered only a non-contrast CT, read it as “negative for acute findings,” and discharged the patient without CTA or MRI, the decision to stop imaging is the decision we litigate. The original study is preserved on the hospital’s PACS system and is re-readable by our neuroradiologists years later.
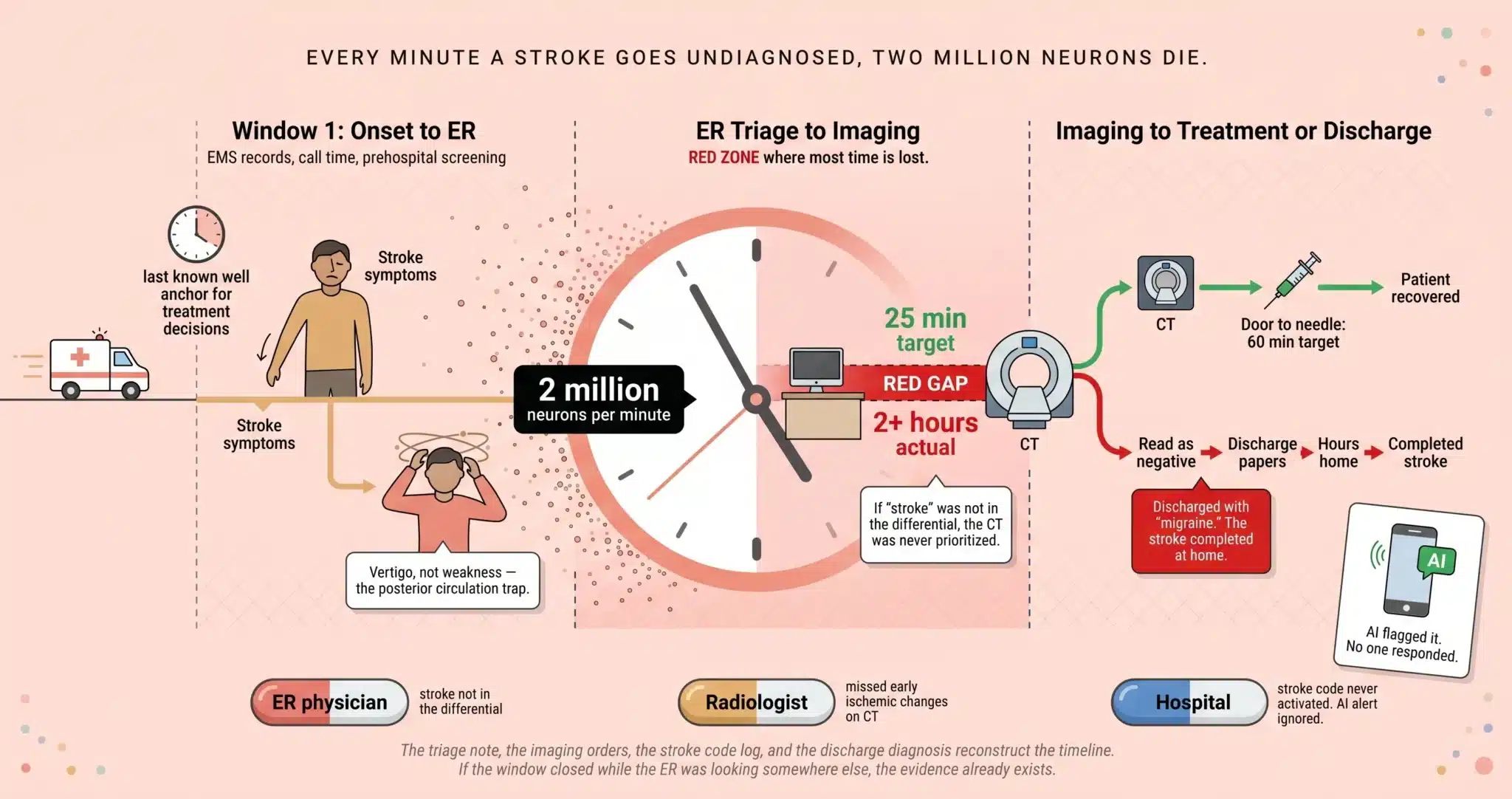
THE FORENSIC STROKE TIMELINE: THREE WINDOWS WHERE MINUTES WERE LOST
Window 1: Symptom Onset to ER Arrival
The “last known well” time is the anchor for every treatment decision that follows. It determines whether the patient is within the 4.5 hour window for tPA or the 24 hour window for mechanical thrombectomy in selected patients. EMS records document the call time, the on-scene assessment, and whether the paramedics classified the event as a possible stroke using a prehospital screening tool. If EMS notified the receiving Miami hospital of a potential stroke patient and the hospital did not have the stroke team assembled on arrival, the failure began before the patient crossed the threshold.
Window 2: ER Triage to Imaging
The AHA/ASA target for door-to-CT is 25 minutes. For door-to-CT interpretation, 45 minutes. In the stroke misdiagnosis cases we handle across Miami-Dade County, the gap between arrival and imaging is often measured in hours, not minutes. The triage nurse assigns a complaint code. The ER physician sees the patient and documents a differential diagnosis. If “stroke” or “CVA” does not appear in that differential, the CT is not ordered with stroke-protocol urgency. The patient is queued behind elective studies. Each timestamp in the electronic record measures the distance between what happened and what should have happened.
Window 3: Imaging to Treatment or Discharge
Once imaging is obtained, the decision tree branches. If the CT shows hemorrhage, the protocol shifts to blood pressure management and neurosurgical consultation. If the CT is negative for hemorrhage and the clinical picture supports ischemic stroke, the team must decide whether to administer tPA (door-to-needle target: 60 minutes) and whether to perform CTA to evaluate for a large vessel occlusion eligible for thrombectomy (door-to-groin puncture target varies by protocol). In the cases we litigate in Miami, the most damaging failure in this window is the decision to discharge. The CT was “negative,” the symptoms “improved,” and the patient was sent home with a diagnosis of migraine or vertigo. Hours later, the stroke completes. The infarct that was small and potentially recoverable at the time of discharge is now large and permanent.
AI DIAGNOSTIC TOOLS: THE NEW NEGLIGENCE ANGLE MOST ATTORNEYS MISS
Multiple Miami hospitals now run AI-assisted imaging platforms that detect intracranial hemorrhage and large vessel occlusions on CT and CTA scans in real time. These systems, including platforms like Viz.ai, flag suspected findings and send alerts directly to the stroke team’s mobile devices before the radiologist has finished the formal read. Published research shows that jurors penalize physicians more when AI identifies a finding the clinician missed, because the technology eliminates the argument that the finding was “subtle” or “easy to overlook.”
When a Miami hospital purchased and installed one of these systems, the question in litigation is no longer limited to whether the individual radiologist or ER physician should have caught the stroke. It extends to whether the institution configured the system correctly, whether the alert was generated, and whether anyone on the clinical team acted on it. If the AI flagged a large vessel occlusion and the on-call neurologist did not respond for 45 minutes, that 45 minutes is attributable to the institution that deployed the tool without ensuring the response chain was functional. Our discovery in stroke cases now routinely includes requests for AI alert logs, notification timestamps, and the hospital’s internal protocols for responding to automated imaging findings.
WHO IS LIABLE WHEN A STROKE IS MISSED
The ER physician who evaluated the patient, documented the differential diagnosis, and made the decision about which imaging to order and when. If stroke was not on the differential and should have been, the ER physician is the primary defendant. The triage nurse who assigned the acuity level and complaint code. If the nurse documented symptoms consistent with stroke and assigned a non-urgent triage category, the delay attributable to that classification belongs to the nurse and the hospital.
The radiologist who read the CT or CTA and either missed early ischemic changes or failed to recommend advanced imaging in the report. The original study is stored on the hospital’s PACS system indefinitely. Our neuroradiologists re-read it. The neurologist who was consulted and either responded too slowly or was never called. The hospital itself for stroke code protocol failures, staffing deficiencies, lack of tele-stroke capability, failure to transfer to a thrombectomy-capable center, or failure to operationalize AI diagnostic tools it had purchased.
WHAT A MISSED STROKE COSTS: THE INJURY, THE RECOVERY, AND THE LIFE CARE PLAN
A stroke that is diagnosed and treated within the window may produce minimal lasting deficits. The same stroke diagnosed hours later, after the treatment window has closed, can produce permanent hemiparesis, expressive or receptive aphasia, visual field cuts, cognitive impairment, personality and behavioral changes, post-stroke epilepsy, depression, and loss of independence. The difference between those two outcomes is the difference between a patient who returns to work and a patient who requires 24 hour attendant care for the rest of their life.
The Life Care Plan in a stroke misdiagnosis case projects the cost of inpatient rehabilitation, outpatient physical therapy, occupational therapy, and speech-language pathology. Neuropsychological testing and cognitive rehabilitation. Anticonvulsant management if post-stroke seizures develop. Assistive devices from ankle-foot orthoses through power wheelchairs. Home modifications for single-sided weakness, accessible bathing, and fall prevention. Modified vehicle or transportation services. Attendant care at the level the patient’s functional deficits require. A forensic economist separately calculates lost income and diminished earning capacity over the patient’s remaining work-life expectancy. The combined projection is built from documented deficits, not speculation.
What the Hospital’s Quality Department Already Knows and Will Not Share Voluntarily
Hospitals track their own stroke metrics. Door-to-CT times. Door-to-needle times. Stroke code activation rates. Percentage of patients screened with the NIH Stroke Scale. These numbers are collected for certification programs like the Joint Commission’s Primary Stroke Center and Comprehensive Stroke Center designations. Attorney Jorge L. Flores knows these internal quality reports exist because he reviewed them during the years he spent at a Miami insurance defense firm representing hospitals. Defense counsel will argue those reports are protected under Florida’s peer review and quality assurance privileges and fight to keep them from the jury.
Jorge Flores knows which categories of quality data are shielded and which are not. He knows that the stroke code activation log, the individual patient’s triage and imaging timestamps, and the AI alert notification records are not peer review materials. They are operational data generated in the ordinary course of patient care. The defense will try to blur the line between quality review and operational records. We draw the line where it belongs and compel production of every document the hospital cannot legitimately withhold.
Two Million Neurons Die Every Minute a Stroke Goes Untreated. The ER Record Tells Us How Many Minutes Were Wasted.
The triage note, the imaging orders, the stroke code log, and the discharge diagnosis reconstruct the timeline. If the window closed while the ER was looking somewhere else, the evidence already exists.
(305) 598-2221
FREQUENTLY ASKED QUESTIONS
Can I sue for stroke misdiagnosis in Miami?+
Yes. If a Miami ER physician failed to diagnose a stroke in time to provide treatment that would have reduced the severity of the injury, and that failure fell below the standard of care, you may have a medical malpractice claim. The case requires expert testimony from a physician in the same specialty establishing that a reasonably competent doctor would have diagnosed the stroke sooner and that earlier treatment would have changed the outcome.
What if my stroke did not look typical? I had vertigo, not weakness.+
Posterior circulation strokes frequently present with vertigo, nausea, difficulty walking, or double vision rather than the classic face-arm-speech symptoms. These presentations are well documented in the medical literature, and ER physicians are trained to consider stroke in their differential when evaluating acute vertigo. If the ER attributed your vertigo to an inner ear condition without performing the HINTS exam or ordering brain imaging, the diagnostic workup may have been inadequate. The chart documents what was considered and what was ruled out.
How do I prove the hospital’s delay made my stroke worse?+
Our neurology experts compare the size of the infarct on the final MRI to what it likely would have been if treatment had been administered at the time it should have been. Published research on tPA and thrombectomy outcomes allows experts to calculate the probability of a better outcome with earlier treatment. The timestamps in the ER record establish when treatment should have been given, and the imaging establishes what was lost during the delay.
Does failure to use or ignoring AI imaging tools count as malpractice?+
The legal framework is evolving, but the principle is straightforward: if a hospital purchased and deployed an AI system designed to detect strokes faster, and that system was not functioning, not configured, or generated an alert that no one acted on, the hospital’s failure to use its own technology is relevant evidence of institutional negligence. It does not replace the standard individual malpractice analysis, but it adds a separate dimension of liability that our investigation routinely explores.
How long do I have to file a stroke misdiagnosis case in Miami?+
Florida’s statute of limitations for medical malpractice is generally two years from the date you knew or should have known the stroke was misdiagnosed, with a four year statute of repose serving as the outer boundary in many cases, though specific deadlines can vary based on the facts and statutes in effect. For wrongful death, the limitations period generally runs two years from the date of death. The ER records, imaging studies, and stroke code logs must be preserved before the hospital’s retention cycle overwrites them. We issue preservation demands immediately upon engagement.
What does it cost to hire a lawyer for a stroke misdiagnosis case?+
We take the financial risk. The ER records, the imaging re-reads by our neuroradiologists, the emergency medicine and neurology expert consultations, the Life Care Plan, and the forensic economics analysis are all funded by this firm. We collect a fee only when compensation is recovered. If the case does not produce a result, every dollar we invested is written off entirely.
CONTACT US FOR A FREE CASE REVIEW
If you or a family member suffered a worsened stroke outcome because a Miami emergency room failed to diagnose it in time, the Law Offices of Jorge L. Flores, P.A., will review the ER records, the imaging, and the clinical timeline at no charge. We tell families what the evidence shows and whether the timestamps support a claim. That conversation costs nothing and commits you to nothing.
Free Case Review. No Cost Unless We Recover Compensation.
We finance the ER record retrieval, the expert consultations, and the full investigation. Our fee is contingent on the outcome.
(305) 598-2221
Related: Medical Malpractice · Wrongful Death · Aortic Dissection Misdiagnosis · Brain & Spinal Cord Injuries