

Former hospital defense attorney · Law Offices of Jorge L. Flores, P.A. · Miami, Florida
Last Updated: April 2026
The Patient Arrived With a Tear in the Aorta. The ER Treated It as Something Else. By the Time the Correct Diagnosis Was Made, the Window Had Closed.
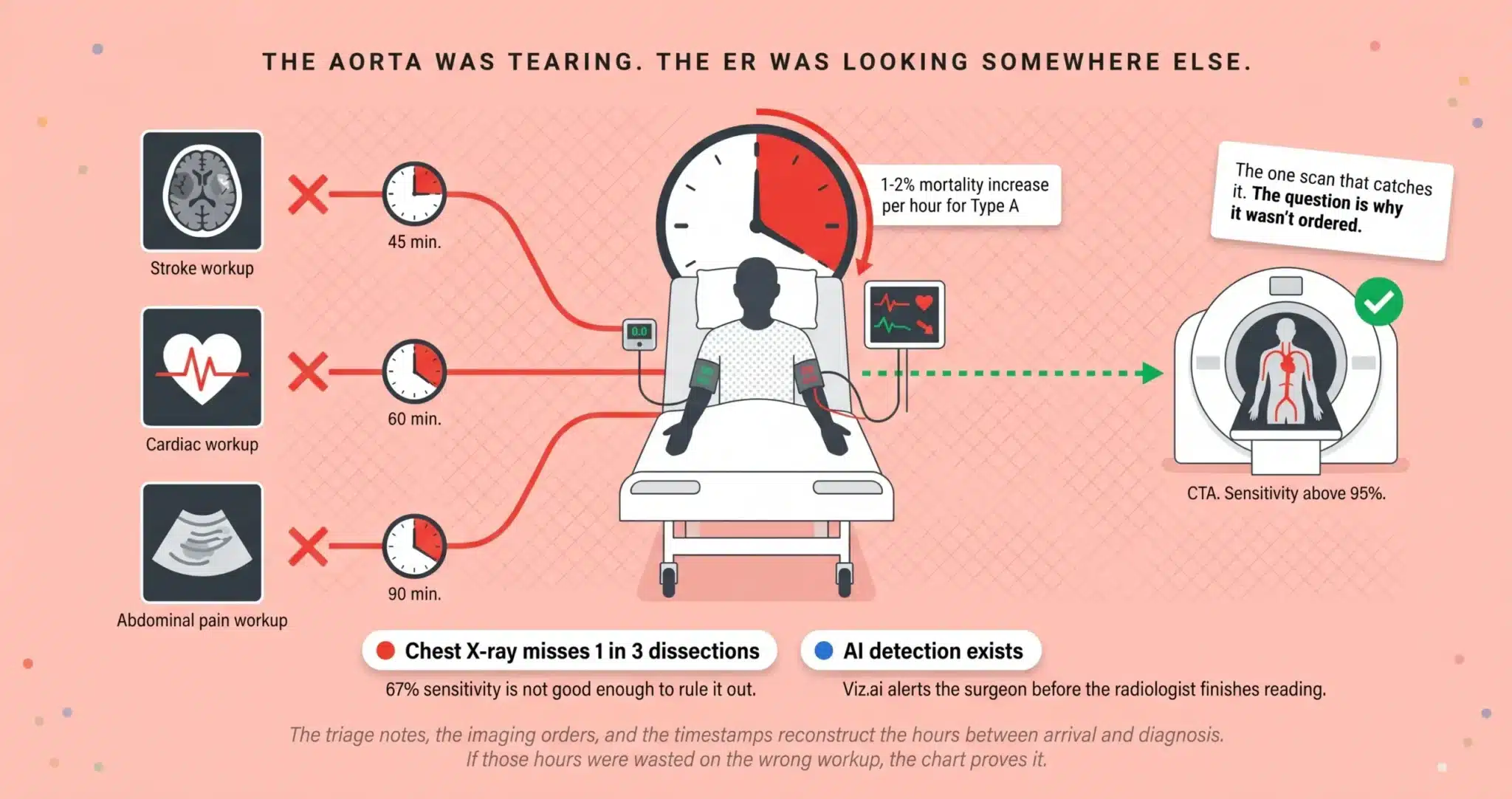
Aortic dissection kills faster than almost any other cardiovascular emergency. A tear opens in the inner wall of the aorta. Blood forces its way between the layers of the vessel wall, creating a false channel that expands with every heartbeat. If the tear involves the ascending aorta, this is a Stanford Type A dissection, and without emergency surgery the mortality rate climbs roughly 1 to 2 percent per hour. A patient who arrives at a Miami emergency room at 6 AM with a Type A dissection and is not in the operating room by 8 AM has lost a measurable percentage of their survival probability for every hour that passed. That is the math the ER team is supposed to know.
The problem is that aortic dissection disguises itself. The textbook presentation is sudden, tearing chest pain radiating to the back. But roughly 6 percent of dissections arrive without pain at all, presenting instead with a stroke, syncope, limb weakness, or abdominal symptoms that send the ER physician down the wrong diagnostic path. The patient gets a head CT for the stroke. A cardiac workup for the syncope. An abdominal ultrasound for the belly pain. And the aorta, which is tearing apart in real time, is never imaged until it ruptures or until the malperfusion has already destroyed the kidneys, the spinal cord, or the brain.
⚠ Every Hour of Delay Costs Survival Probability
If your family member died from or was permanently injured by an aortic dissection that a Miami emergency room failed to diagnose in time, the ER triage notes, the imaging orders, and the timestamps on every test tell us exactly how many hours were lost and whether a CT angiography should have been ordered sooner. Florida’s statute of limitations for medical malpractice is generally two years from the date of discovery, and wrongful death claims generally run two years from the date of death, though specific deadlines can vary based on the facts and statutes in effect.
The Dissection May Have Been Missed If:
✓ Your family member arrived at the ER with sudden chest pain, back pain, or syncope and was initially worked up for a heart attack or stroke.
✓ A chest X-ray was performed but a CT angiography was not ordered despite ongoing or worsening symptoms.
✓ Neurological deficits, limb weakness, or loss of pulse in an extremity developed while the patient was still in the ER.
✓ Hours passed between the initial ER arrival and the point at which the aortic dissection was finally identified on imaging.
✓ The patient was discharged from the ER and returned or died before the dissection was diagnosed.
If any of these describe what happened, the ER records, the imaging orders, and the timestamps deserve an independent review. We arrange that review at no cost to your family.
On This Page
Why the ER Missed It: The Diagnostic Failures That Turn a Survivable Tear Into a Fatal One
Malperfusion: What Happens to the Body While the Aorta Goes Undiagnosed
The Technology That Should Have Caught It and the Question of Whether It Was Used
Surviving a Missed Dissection: The Long Road and What It Costs
WHY THE ER MISSED IT: THE DIAGNOSTIC FAILURES THAT TURN A SURVIVABLE TEAR INTO A FATAL ONE
The Chest X-Ray Trap: 67% Sensitivity Is Not Good Enough to Rule It Out
The most common diagnostic failure we see in Miami aortic dissection cases is the ER physician who orders a chest X-ray, sees a widened mediastinum or does not see one, and moves on. A chest X-ray detects aortic dissection in roughly two out of three cases. That means one in three dissections look normal on the film. The definitive imaging study is CT angiography of the chest, which has a sensitivity above 95 percent and can identify the location of the tear, the extent of the dissection flap, and which branch vessels are compromised. When a patient presents with acute onset chest or back pain, a blood pressure differential between arms, a new aortic regurgitation murmur, or a pulse deficit, the question is not whether the chest X-ray was reassuring. The question is why the CTA was not ordered.
The Painless Dissection: When the Aorta Tears Without the Textbook Symptoms
Approximately 6.4 percent of acute aortic dissections present without chest or back pain. The International Registry of Acute Aortic Dissection (IRAD) documented this in a cohort study that found painless dissections are more common in patients with diabetes, prior aortic aneurysm, or prior cardiac surgery. These patients arrive at the ER with a stroke, with syncope, with acute limb ischemia, or with renal failure, and the ER physician treats the presenting symptom without considering that all of them trace back to a single catastrophic event in the aorta. The patient receives a head CT for the stroke. A Foley catheter for the renal failure. A vascular consult for the cold leg. And the dissection continues to propagate while the team chases its consequences instead of its cause.
The Clinical Red Flags the ER Should Have Caught
Blood pressure readings that differ by more than 20 mmHg between the left and right arms. An absent or diminished pulse in one extremity. A new diastolic murmur consistent with aortic regurgitation. Rising lactate levels that suggest tissue ischemia despite a seemingly stable presentation. A D-dimer that returns markedly elevated. Each of these findings is documented in the ER chart. Each one should have triggered the ER physician to consider aortic dissection in the differential diagnosis and order the CTA that would have confirmed it. When the chart shows these findings were present, documented by the nursing staff, and not acted upon by the physician, the failure is not a matter of medical judgment. It is a failure to connect findings that any board-certified emergency physician should have recognized as pointing toward a single diagnosis.
MALPERFUSION: WHAT HAPPENS TO THE BODY WHILE THE AORTA GOES UNDIAGNOSED
A dissection does not just threaten the aorta. As the false channel expands, it can compress or occlude the branch arteries that supply blood to the brain, the spinal cord, the kidneys, the intestines, and the limbs. This is called malperfusion, and it is responsible for the devastating secondary injuries that make aortic dissection cases some of the highest-value malpractice claims in Miami-Dade County.
Cerebral malperfusion occurs when the dissection flap extends into the carotid or vertebral arteries. The patient suffers a stroke, not from atherosclerosis, but from mechanical obstruction caused by a tear the ER failed to identify. Spinal cord malperfusion produces paraplegia when the intercostal arteries that feed the anterior spinal artery are compromised. Renal malperfusion causes acute kidney failure. Mesenteric malperfusion produces bowel ischemia that can progress to necrosis if not recognized surgically. Limb malperfusion presents as a cold, pulseless extremity that may require amputation. Each of these injuries is a separate element of damages. Each one can be traced, through the imaging and the clinical timeline, to the interval during which the dissection was present but undiagnosed.
THE TECHNOLOGY THAT SHOULD HAVE CAUGHT IT AND THE QUESTION OF WHETHER IT WAS USED
A growing number of Miami hospitals have deployed AI-driven imaging prioritization platforms such as Viz.ai that flag suspected aortic emergencies on CT scans and immediately alert the on-call vascular or cardiothoracic surgeon before the radiologist has even finished reading the study. These systems are designed to eliminate the diagnostic delay that kills patients. The algorithm identifies the dissection flap on the CTA, sends a notification to the surgical team’s mobile device, and compresses the interval between imaging and intervention from hours to minutes.
When a hospital has this technology installed and either did not use it, did not configure it correctly, or did not act on the alert it generated, the failure takes on a different dimension. It is no longer a physician who missed a subtle finding. It is an institution that purchased a system designed to prevent exactly this outcome and then failed to operationalize it. Our investigation in aortic dissection cases now includes discovery into whether the hospital had AI-assisted imaging prioritization available, whether the system was active at the time of the patient’s scan, and whether the alert was generated and ignored.
SURVIVING A MISSED DISSECTION: THE LONG ROAD AND WHAT IT COSTS
Patients who survive a missed aortic dissection face a recovery that extends for years, and a set of lifelong medical requirements that the defense will minimize if your attorney allows them to. The initial repair, whether open surgical graft replacement for Type A or endovascular stent graft for Type B, is only the beginning. Reoperation rates for aortic dissection are substantial. The dissected segment can dilate over time, forming an aneurysm that requires surveillance imaging every six to twelve months for the rest of the patient’s life. Blood pressure must be maintained below aggressive targets, often requiring multiple antihypertensive medications with ongoing titration and monitoring.
If malperfusion produced a stroke, the patient may require inpatient rehabilitation, speech therapy, physical therapy, occupational therapy, and cognitive rehabilitation for months or years. If spinal cord ischemia caused paraplegia, the cost projection includes wheelchair equipment, home accessibility modifications, vehicle adaptation, and attendant care. If kidney failure resulted, the patient may require dialysis or transplant evaluation. A Life Care Planner who specializes in catastrophic vascular injury projects each of these needs across the patient’s remaining life expectancy, and a forensic economist calculates the lost income and diminished earning capacity. The total is built from documented medical necessity, not from rhetoric.
What the Hospital’s Legal Team Is Doing Right Now That Most Plaintiff Attorneys Never See
The courtroom arguments are the part everyone expects. What most families never learn is that the defense wins aortic dissection cases months before trial through tactics that happen in conference rooms and IT departments. Attorney Jorge L. Flores knows this because he executed these tactics during the years he spent at a Miami insurance defense firm representing hospitals.
The first move is records. Emergency departments store electronic data on systems with automatic overwrite cycles. The Viz.ai alert log, the radiology worklist showing when the CTA was ordered versus when it was read, the ER tracking board showing how many patients were ahead of yours, the triage nurse’s electronic timestamp on the initial assessment: all of this exists on servers that the hospital controls. If no preservation demand is filed early, that data can be overwritten or archived into a format the hospital claims is “no longer retrievable.” Jorge Flores knows exactly which data fields to demand and the specific language required in a Florida statutory preservation request to prevent the hospital from claiming the records were lost to routine system maintenance.
The second move is expert exclusion. Defense counsel in ER misdiagnosis cases will file Daubert motions to disqualify the plaintiff’s emergency medicine expert on the grounds that the expert’s methodology does not reflect “real world ER conditions” or that the expert has not practiced emergency medicine in the last five years. Jorge Flores filed these motions himself. He knows what makes an expert vulnerable to exclusion and what makes one bulletproof. Every expert we retain for an aortic dissection case is selected to survive the challenge he once would have prepared against them.
The Aorta Was Tearing. The ER Was Looking Somewhere Else. The Chart Shows Exactly Where the Investigation Went Wrong.
The triage notes, the imaging orders, the timestamps, and the vital sign trends reconstruct the hours between arrival and diagnosis. If those hours were wasted on the wrong workup, the evidence already exists in the chart.
(305) 598-2221
FREQUENTLY ASKED QUESTIONS
What is the difference between a Type A and Type B aortic dissection?+
The Stanford classification divides aortic dissections by location. Type A involves the ascending aorta and is a surgical emergency requiring immediate open repair. Type B involves only the descending aorta and may be managed medically with aggressive blood pressure control, though complicated Type B dissections with malperfusion also require urgent intervention. In malpractice litigation, the classification determines what the standard of care required and how quickly the surgical team should have been mobilized.
Can an aortic dissection be missed on a chest X-ray?+
Yes. A chest X-ray detects aortic dissection in approximately 67 percent of cases. One in three dissections present with a normal appearing mediastinum on the film. CT angiography is the definitive study, with sensitivity above 95 percent. When a Miami ER physician relied on a chest X-ray to exclude dissection and did not order the CTA, and the patient subsequently ruptured or developed malperfusion, the reliance on an insufficient test is a central element of the negligence claim.
What is malperfusion and why does it matter for my case?+
Malperfusion occurs when the expanding dissection flap blocks blood flow to organs supplied by the aorta’s branches. It can produce stroke, paraplegia, kidney failure, bowel necrosis, or limb ischemia requiring amputation. Each malperfusion injury is a separate category of damages. The imaging timeline shows when the dissection was present and when each organ began losing blood supply, allowing our experts to calculate the window during which diagnosis and intervention would have prevented the secondary injury.
Do hospitals have AI that can detect aortic dissections automatically?+
A growing number of hospitals use AI platforms such as Viz.ai that analyze CT scans in real time and alert the surgical team when a suspected aortic emergency is detected. If the hospital had this technology installed and it was not active, not configured, or the alert was generated and not acted upon, that institutional failure adds a separate dimension to the negligence claim beyond the individual physician’s diagnostic error.
My family member died from a missed dissection. Can I still file a claim?+
Yes. Florida’s wrongful death statute allows surviving family members to bring a claim. The statute of limitations for wrongful death generally runs two years from the date of death, though specific deadlines can vary based on the facts and statutes in effect. The ER records, the imaging studies, the lab results, and the autopsy report (if performed) reconstruct the timeline and establish whether earlier diagnosis would have changed the outcome. We retain board-certified emergency medicine physicians and cardiothoracic surgeons who evaluate the standard of care and testify to what should have been done differently.
What does it cost to hire an attorney for an aortic dissection case?+
We carry every cost of the case from the initial record request through expert depositions and trial preparation. The ER records, the radiology images, the emergency medicine expert review, the cardiothoracic surgical consultation, and the Life Care Plan are all funded by our firm. We collect a fee only when compensation is recovered for your family. If the case does not produce a result, the financial risk was entirely ours.
CONTACT US FOR A FREE CASE REVIEW
If your family member was misdiagnosed, discharged, or lost to an aortic dissection that a Miami emergency room should have caught, the Law Offices of Jorge L. Flores, P.A., will review the ER records, the imaging orders, and the clinical timeline at no charge. We tell families what the evidence shows. That conversation carries no obligation.
Free Case Review. No Cost Unless We Recover Compensation.
We finance the investigation, the medical experts, and the economic analysis. Our fee is contingent on the outcome.
(305) 598-2221
Or submit your information below and we will contact you within 24 hours.
Your information is confidential. Submitting this form does not create an attorney-client relationship.
Prefer to speak directly? Call (305) 598-2221 for an immediate consultation.
Related: Medical Malpractice · Wrongful Death · Brain & Spinal Cord Injuries