

Former hospital defense attorney · Law Offices of Jorge L. Flores, P.A. · Miami, Florida
Last Updated: April 2026
Neonatal Seizures Are Not a Diagnosis. They Are a Symptom That Something Went Wrong During Delivery.
If your baby is in a Miami NICU right now and the medical team has mentioned seizures, you are reading this at one of the worst moments of your life. The monitors are beeping. The nurses are adjusting medications. Someone may have used the phrase “we are watching for seizure activity.” What no one in that room is telling you is that neonatal seizures in a full-term infant are rarely spontaneous. They are almost always the brain’s response to an injury that occurred during labor and delivery. The injury has a name. It is called hypoxic-ischemic encephalopathy, or HIE, and it means the baby’s brain was deprived of oxygen at a point when intervention could have prevented the damage.
The seizures are the alarm. The question your family needs answered is what set the alarm off and whether the medical team had the opportunity to prevent it. That is not a medical question. That is a legal one. And the answer is inside the fetal monitoring strips, the delivery room records, and the NICU admission notes that are being generated right now in the room where your baby is being treated.
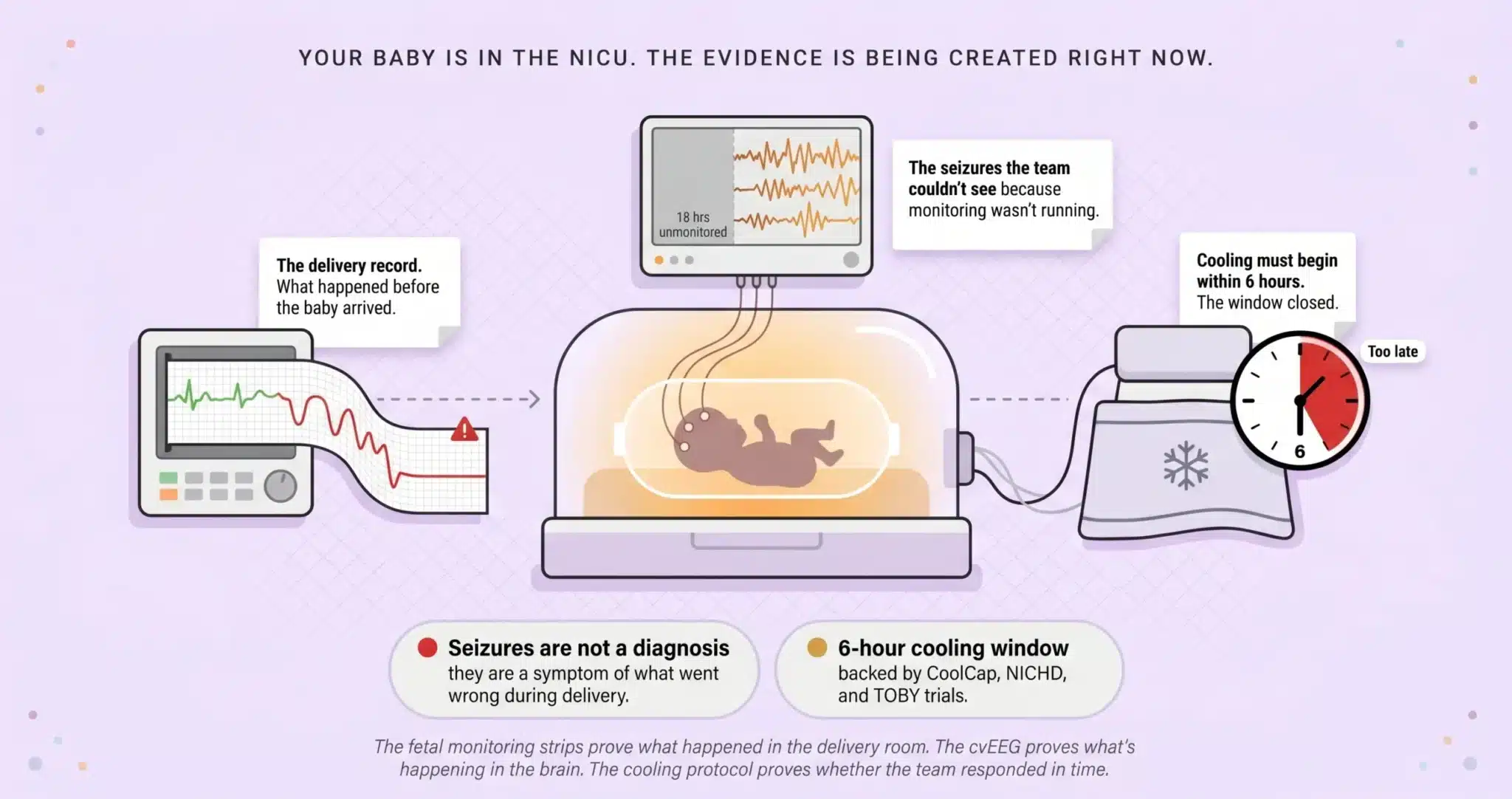
⚠ Your Baby Is in the NICU. The Evidence Is Being Created Right Now.
Florida law gives families two years from the date of discovery to file a medical malpractice claim. In many Florida birth injury cases, the limitations period extends until around the child’s eighth birthday, though specific deadlines depend on the facts and statutes in effect. But the continuous video EEG data, the fetal monitoring strips, and the delivery room nursing notes are stored on the hospital’s retention schedule. Securing these records early is critical.
Free Case Review: Was the Seizure Preventable? (305) 598-2221
Your Baby’s Seizures May Be the Result of a Preventable Injury If:
✓ The fetal heart rate monitor showed recurrent late decelerations, prolonged decelerations, or minimal variability during labor.
✓ Apgar scores were low at one and five minutes and the baby required resuscitation at birth.
✓ Your baby was admitted to the NICU and seizure activity was identified hours or days after delivery.
✓ Therapeutic hypothermia (cooling) was not offered or was started more than six hours after birth.
✓ Continuous video EEG monitoring was not initiated in the first hours of the NICU admission.
If any of these describe what happened during your delivery or your baby’s NICU stay, the fetal monitoring strips and the NICU records deserve an independent medical review. We arrange that review at no cost to your family.
On This Page
The Delivery Room Failures That Cause Neonatal Seizures
Continuous Video EEG: The Evidence the NICU Is Generating Right Now
The Diagnostic Timeline: When the Seizure Should Have Been Caught Versus When It Was
THE DELIVERY ROOM FAILURES THAT CAUSE NEONATAL SEIZURES
Other law firm websites define seizures. They describe what they look like. They list causes. None of that tells you whether your child’s seizures were the result of something preventable. To answer that, we trace the seizure backward through the medical record to the event that triggered it. In the majority of full-term neonatal seizure cases we handle in Miami, that event falls into one of three categories.
Oxygen Deprivation During Labor: Hypoxic-Ischemic Encephalopathy (HIE)
HIE is the leading cause of neonatal seizures in full-term infants. It occurs when blood flow or oxygen delivery to the fetal brain is interrupted during labor. The electronic fetal monitor records the baby’s heart rate continuously throughout labor. When the tracing shows late decelerations, prolonged decelerations, or minimal variability, the clinical team is looking at a brain that is running out of oxygen reserve.
The question is not whether the tracing deteriorated. The question is what the obstetric team did with the information the monitor was giving them, and how much time passed between the first nonreassuring pattern and the decision to deliver. In our experience litigating these cases across Miami-Dade County, the fetal heart rate strips are the single most important piece of evidence. Our maternal-fetal medicine experts re-read them tracing by tracing, annotate every deceleration pattern, and calculate whether the clinical response matched the urgency the pattern demanded.
Untreated Maternal Infection: When Inflammation Reaches the Fetal Brain
Group B Streptococcus, chorioamnionitis, and other intrauterine infections produce inflammatory cytokines that cross the placenta and damage developing neural tissue. The maternal chart records the temperature, the white blood cell count, and the clinical findings that should have triggered antibiotic administration or expedited delivery. When the infection markers were documented and the obstetric team delayed the response, the interval between the first clinical sign and the first intervention is measurable, documented, and central to the case.
Traumatic Delivery: Instrument Injuries and Shoulder Dystocia
Forceps that compressed the skull. A vacuum extractor that caused a subgaleal hemorrhage. A shoulder dystocia where excessive traction on the head produced a brachial plexus injury alongside intracranial bleeding. These mechanical injuries can trigger seizures within hours of delivery. The operative note describes what instruments were used, how many attempts were made, and how much force was applied. When the documentation reveals that a vacuum was popped off three times and reapplied, or that fundal pressure was used during a shoulder dystocia in violation of current ACOG guidance, the mechanism connecting the delivery technique to the seizure is direct and provable.
CONTINUOUS VIDEO EEG: THE EVIDENCE THE NICU IS GENERATING RIGHT NOW
Continuous video EEG, sometimes abbreviated cvEEG, is the gold standard for detecting neonatal seizures. Many seizures in newborns are subclinical. The baby does not convulse. The baby does not shake. The electrical activity is happening inside the brain without any visible manifestation, and only the EEG captures it. The concept of “seizure burden,” the total volume of seizure activity over a given period, is what neonatal neurologists use to assess the severity of the brain injury and guide treatment with anticonvulsant medications like phenobarbital or levetiracetam.
From a legal standpoint, the cvEEG record is a second timeline running parallel to the delivery records. It tells us when the seizures started, how frequent they were, how long each one lasted, and whether the NICU team responded to the electrographic findings in real time or whether hours of subclinical seizure activity went unrecognized because the monitoring was not being read by a qualified neurophysiologist. In Miami, we obtain the raw EEG data and retain pediatric neurologists who re-read every hour of the recording to determine whether the seizure burden was identified and treated with the urgency it required.
THE DIAGNOSTIC TIMELINE: WHEN THE SEIZURE SHOULD HAVE BEEN CAUGHT VERSUS WHEN IT WAS
No competitor in the current SERP provides a diagnostic timeline showing the gap between when a seizure should have been identified and when the clinical team actually recognized it. That gap is where cases are built.
A baby is born following a difficult labor marked by recurrent late decelerations. Apgar scores are low at one and five minutes. The infant is admitted to the NICU. If the hospital follows the standard of care for a newborn with suspected HIE, continuous video EEG monitoring should begin within the first few hours of life, and therapeutic hypothermia (cooling) should be initiated within six hours of birth to limit the extent of the brain injury.
Now consider what happens when the standard is not met. The baby is admitted. The NICU team orders routine monitoring but does not initiate cvEEG for 18 hours. During those 18 hours, the baby is experiencing electrographic seizures that nobody sees because there is no EEG running. Cooling, which has a strict six hour initiation window supported by the landmark CoolCap, NICHD, and TOBY trials, is not started because the clinical team did not classify the injury as moderate to severe HIE in time. When our pediatric neurology experts review the case, they reconstruct what the EEG would have shown during those missing 18 hours based on the clinical trajectory and the subsequent EEG findings. The seizure burden that accumulated during the gap is brain damage that did not have to happen.
WHAT THE NEXT TWENTY YEARS WILL COST AND HOW WE PROVE IT
Neonatal seizures caused by HIE frequently produce cerebral palsy, epilepsy requiring lifelong anticonvulsant management, cognitive and developmental delays, and feeding difficulties that may require a gastrostomy tube. The severity depends on the extent of the hypoxic injury and the seizure burden in the first days of life. A child with mild HIE may develop learning disabilities that become apparent in elementary school. A child with severe HIE may never walk, speak, or feed independently.
The Life Care Plan we commission for each case is built by a certified planner who evaluates the child’s specific deficits and projects every category of need across the full life expectancy. Physical therapy, occupational therapy, speech therapy, and cognitive rehabilitation with frequency schedules that evolve as the child grows. Anticonvulsant medication management and neurology follow up for decades. Adaptive equipment from infant positioning systems through adult power wheelchairs. Specialized schooling, tutoring, and vocational support. Home modifications and accessible transportation. Attendant care at the level the child’s functional limitations require. A vocational economist independently calculates the income the child would have generated across a working career absent the injury. Combined, these projections produce an evidence-based number that a jury can evaluate against specific line items rather than an abstract appeal to sympathy.
The Attorney Who Prepared These Defense Arguments Before He Switched Sides
The hospital will call the seizures “idiopathic.” Their neonatologist will testify that the fetal heart rate tracing was “Category II and reassuring.” Their expert will argue that the cooling window was not missed because the injury “did not meet the criteria for therapeutic hypothermia.” Attorney Jorge L. Flores knows these arguments because he drafted versions of them during the years he spent at a Miami insurance defense firm representing hospitals against birth injury claims.
He learned which arguments hold up and which ones fracture under a properly prepared cross examination. A “Category II” tracing that persisted for 90 minutes without intervention is not reassuring. It is a tracing that required action. “Idiopathic” seizures in a baby born after a labor complicated by recurrent decelerations and low Apgars are not idiopathic. They are the predictable neurological consequence of oxygen deprivation that the monitoring system was designed to detect. Jorge Flores builds every neonatal seizure case to close the exits the defense relies on.
The Seizure Is the Alarm. The Delivery Record Explains What Triggered It.
The fetal monitoring strips, the NICU admission notes, the cvEEG data, and the cooling protocol documentation reconstruct the full picture. If the team had the information and did not act on it, the evidence already exists.
(305) 598-2221
FREQUENTLY ASKED QUESTIONS
What are the first signs of a birth injury seizure?+
In newborns, seizures often do not resemble the convulsions adults associate with the word. A neonatal seizure may present as subtle eye movements, lip smacking, cycling motions of the legs, or episodes of apnea (pauses in breathing). Many seizures are entirely subclinical, visible only on continuous video EEG. That is why cvEEG monitoring in the NICU is the gold standard: it captures seizure activity the clinical staff cannot see with their eyes.
What is HIE and how is it connected to neonatal seizures?+
Hypoxic-ischemic encephalopathy is brain injury caused by oxygen deprivation during labor and delivery. It is the most common cause of seizures in full-term newborns. The oxygen deprivation damages neurons, and the damaged neurons produce abnormal electrical discharges that manifest as seizures on the EEG. The severity of the HIE, classified as mild, moderate, or severe based on clinical criteria and imaging, determines both the seizure burden and the long-term neurological outcome.
What is therapeutic hypothermia and why does the timing matter?+
Therapeutic hypothermia, or “cooling,” is a neuroprotective treatment where the baby’s body temperature is lowered to 33.5 degrees Celsius for 72 hours. It must be initiated within six hours of birth to be effective. The landmark clinical trials, including the CoolCap, NICHD, and TOBY studies, established this window. If a Miami hospital did not begin cooling within six hours because the team failed to classify the injury as moderate to severe HIE in time, the delay is a departure from a protocol backed by the highest level of clinical evidence.
Can my baby’s seizures cause additional brain damage beyond the original injury?+
Yes. There is growing evidence that prolonged or recurrent neonatal seizures cause secondary brain injury independent of the original insult. This is why seizure burden matters. An infant experiencing electrographic seizures that go undetected for hours because cvEEG was not initiated, or because the EEG data was not being interpreted in real time, may sustain additional damage that proper monitoring would have prevented. That secondary injury is a separate element of the negligence claim.
How long do I have to file a neonatal seizure birth injury case in Miami?+
In many Florida birth injury cases, the filing deadline does not arrive until around the child’s eighth birthday, though specific deadlines depend on the facts and statutes in effect at the time of the injury. But the cvEEG data, the fetal monitoring strips, the NICU flowsheets, and the cooling protocol documentation are maintained on the hospital’s retention schedule. If those files are purged before your attorney requests them, the strongest evidence in the case may be gone. Contacting us early allows us to issue preservation demands while the records are still intact.
What does it cost to hire a lawyer for a neonatal seizure case?+
We carry the entire financial burden of the case from the first record request through the final expert deposition. The medical record retrieval, the EEG interpretation by our pediatric neurologists, the neuroradiology review of the MRI, the Life Care Plan, the vocational economics analysis: all of it is funded by our firm. We collect a fee only if compensation is recovered. If the case does not produce a result, every dollar we invested is absorbed by us.
CONTACT US FOR A FREE CASE REVIEW
If your newborn is experiencing seizures in a Miami NICU or has been diagnosed with HIE following a difficult delivery, the Law Offices of Jorge L. Flores, P.A., will review the delivery and NICU records at no charge. We tell families what the evidence shows and whether it supports a claim. That conversation costs nothing and commits you to nothing.
Free Case Review. No Cost Unless We Recover Compensation.
We fund the investigation, the medical experts, and the Life Care Plan. Our fee comes from the result, not from your family.
(305) 598-2221
Related: Birth Injuries · Brain & Spinal Cord Injuries · Periventricular Leukomalacia (PVL) · Kernicterus · Umbilical Cord Prolapse · Medical Malpractice