

Former hospital defense attorney · Law Offices of Jorge L. Flores, P.A. · Miami, Florida
Last Updated: April 2026
The Fetal Monitor Was Showing Distress. The Decision to Deliver Should Have Come Sooner. The Minutes That Passed Are Documented.
A delayed cesarean section case is not about whether a C-section was eventually performed. It is about whether it was performed in time.
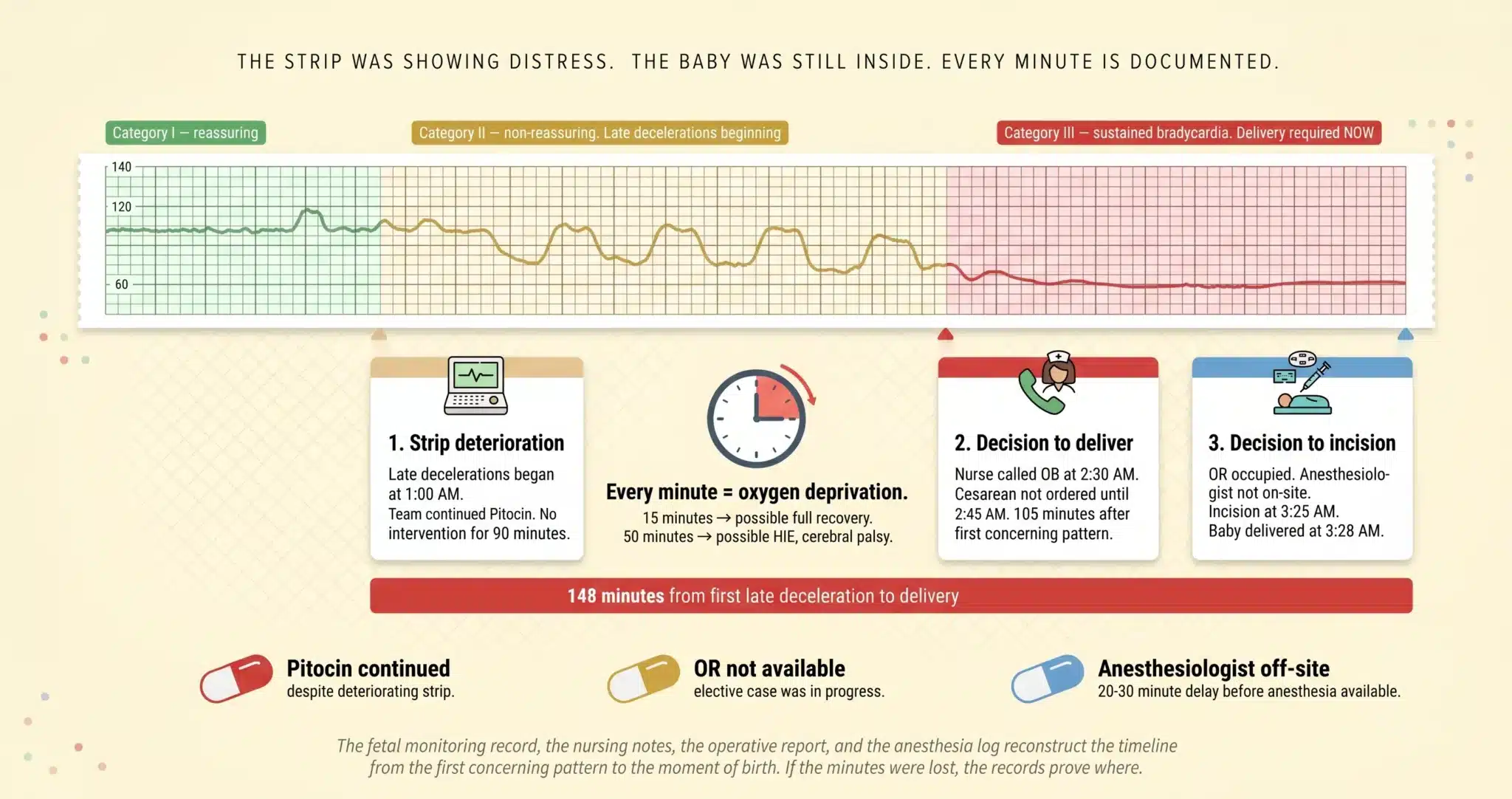
The fetal heart rate monitor runs continuously during labor. It records every acceleration, every deceleration, every period of variability or absence of variability. When the tracing deteriorates from Category I to Category II to Category III, the information the obstetric team needs to make the decision is on the screen in front of them. The question in every case we handle in Miami is not whether the strip looked concerning. The question is how many minutes passed between the point when the strip demanded delivery and the moment the baby was actually born.
Those minutes are not abstract. They are the minutes during which the baby’s brain was deprived of oxygen. A baby delivered 15 minutes after the strip showed sustained bradycardia may recover fully. The same baby delivered 50 minutes later may have hypoxic ischemic encephalopathy, cerebral palsy, or may not survive.
The difference between those two outcomes is documented in the fetal monitoring record, the nursing notes, the operative report, and the anesthesia log. The records do not guess. They timestamp.
⚠ The Fetal Monitoring Strips Are the Central Evidence. They Must Be Preserved.
In many Florida birth injury cases, the limitations period for a minor does not begin to run until around the child’s eighth birthday, though specific deadlines can depend on the facts and statutes in effect. The fetal monitoring strips, the labor nursing notes, the operative report, and the anesthesia record are stored on the hospital’s retention schedule and can be purged if not preserved early.
Free Case Review: Should Delivery Have Come Sooner? (305) 598-2221
You May Have a Delayed C-Section Case If:
✓ The fetal heart rate monitor showed recurrent late decelerations, prolonged decelerations, minimal or absent variability, or sustained bradycardia and a C-section was not called or performed promptly.
✓ Labor was complicated by placental abruption, uterine rupture, or cord prolapse and minutes or hours passed before an emergency cesarean was initiated.
✓ Vacuum or forceps were attempted multiple times before switching to a C-section, and your baby was born with seizures, HIE, or cerebral palsy.
✓ Pitocin was continued despite a deteriorating fetal heart rate tracing instead of being stopped and delivery expedited.
✓ You were told afterward that “we should have gone to the C-section sooner” or that the operating room, the anesthesiologist, or the surgical team was not available when needed.
If any of these describe your delivery experience at a Miami hospital, the fetal monitoring strips and the operative timeline deserve an independent review. We arrange that review at no cost to your family.
On This Page
The Clinical Scenarios Where Delay Is Most Often Negligent
The Fetal Monitoring and Delivery Timeline: Three Windows Where Minutes Were Lost
Staffing Gaps, OR Delays, and the Institutional Failures Behind the Lost Minutes
What a Delayed C-Section Does to the Baby and What It Costs for a Lifetime
THE CLINICAL SCENARIOS WHERE DELAY IS MOST OFTEN NEGLIGENT
Persistent Non-Reassuring Fetal Heart Rate
Recurrent late decelerations that do not resolve with maternal repositioning and fluid bolus. Prolonged decelerations lasting more than two minutes. A sinusoidal pattern. Minimal or absent variability persisting for more than 60 minutes. These are Category III findings or sustained Category II patterns that require intervention. The fetal monitoring strip records them in real time. When these patterns appear and the obstetric team continues to observe, continues Pitocin, or delays the call for a cesarean, every additional minute on the strip is a minute of documented inaction.
Placental Abruption and Uterine Rupture
Placental abruption separates the placenta from the uterine wall before delivery. The mother experiences sudden severe abdominal pain, vaginal bleeding, and a rigid uterus. The fetal heart rate drops. Uterine rupture, particularly in patients attempting vaginal birth after cesarean (VBAC), produces a similar emergency: sudden pain, loss of fetal station, maternal tachycardia and hypotension, and fetal bradycardia.
Both require crash cesarean delivery measured in minutes, not the standard 30 minute benchmark. In the delayed C-section cases we handle in Miami, the gap between the first sign of abruption or rupture and the delivery of the baby is the variable our experts measure against published survival and neurological outcome data.
Failed Induction, Pitocin Mismanagement, and Prolonged Labor
Pitocin augments contractions. When contractions become too frequent (tachysystole) or too intense, the uterus does not relax between them, and blood flow to the baby is compromised. The fetal heart rate tracing reflects this in real time. The standard of care requires the team to reduce or stop Pitocin when the strip deteriorates and to move to cesarean delivery when the labor is not progressing despite augmentation and the fetal status is non-reassuring.
In the cases we litigate across Miami-Dade County, the most common failure in this scenario is the team that continues Pitocin for hours after the strip has shown the baby is not tolerating the contractions. The medication administration record documents every dose increase, every decrease, and every time the drip was stopped and restarted. Laid alongside the fetal monitoring strip, those records show whether the team was managing the labor or simply waiting for the baby to deliver vaginally at a cost the brain could not afford.
THE FETAL MONITORING AND DELIVERY TIMELINE: THREE WINDOWS WHERE MINUTES WERE LOST
Window 1: Strip Deterioration
Our maternal-fetal medicine experts re read the entire fetal monitoring strip from admission to delivery. They annotate the transition points: when the tracing moved from reassuring to non-reassuring, when the first concerning pattern appeared, how long it persisted, and whether it worsened over time. The strip is not a single snapshot. It is a continuous record that captures the baby’s status minute by minute. The defense will cherry pick 30 second segments that look acceptable. We present the full trajectory.
Window 2: The Decision to Deliver
The interval between the first non-reassuring strip and the physician’s documented decision to proceed to cesarean delivery is the most contested segment of the timeline. The nursing notes record when the nurse called the obstetrician. The physician’s note records when they evaluated the patient. The order log records when the cesarean was officially called. If the nurse documented recurrent late decelerations at 1:00 AM and the physician did not order the cesarean until 2:45 AM, those 105 minutes are in the record.
Window 3: Decision to Incision and Delivery
Once the cesarean is called, the institutional clock starts. The OR must be available. The anesthesiologist must be present. The surgical team must be assembled. The anesthesia record documents when the patient arrived in the OR, when anesthesia was administered, and when the incision was made. The operative report documents when the baby was delivered. For emergent cesareans, many Miami hospitals target 30 minutes from decision to incision. For crash scenarios like abruption, rupture, or sustained bradycardia, 30 minutes may be far too long. Our experts compare the actual interval against what the clinical urgency demanded, not against a fixed institutional benchmark.
STAFFING GAPS, OR DELAYS, AND THE INSTITUTIONAL FAILURES BEHIND THE LOST MINUTES
No available operating room. The OR was occupied by an elective procedure when the emergency cesarean was called. The mother waited in the labor room while the baby’s heart rate remained in the 60s. The OR schedule, the surgical log, and the anesthesia records from the concurrent case document whether the hospital had the capacity to respond to the emergency and whether the delay was caused by a scheduling decision the institution made hours earlier.
Anesthesiologist not on site. Some Miami hospitals do not require a dedicated obstetric anesthesiologist to be physically present in the building around the clock. When an emergency cesarean is called at 3 AM and the anesthesiologist has to drive in from home, the 20 to 30 minutes that pass before anesthesia is available are minutes of continued oxygen deprivation. The call log, the anesthesia arrival time, and the interval between the patient reaching the OR and the induction of anesthesia are all documented.
Chain of command failures. The labor nurse recognized the deteriorating strip and called the on-call obstetrician. The obstetrician gave telephone orders to reposition the mother and administer oxygen but did not come to the bedside. The nurse called again 30 minutes later. The physician still did not come. The charge nurse finally escalated to the department chief. By the time the cesarean was performed, the baby had been in distress for over an hour. The nursing notes, the call log, and the physician response times document every link in the chain and every link that broke.
WHAT A DELAYED C-SECTION DOES TO THE BABY AND WHAT IT COSTS FOR A LIFETIME
Oxygen deprivation during labor produces hypoxic-ischemic encephalopathy, the brain injury that leads to cerebral palsy, seizures, developmental delays, feeding difficulties, and in severe cases, death. The severity correlates with the duration and depth of the oxygen deprivation. A baby who experienced 10 minutes of severe bradycardia before delivery may have mild HIE and recover with therapeutic hypothermia. A baby who experienced 45 minutes of the same pattern may have severe HIE, quadriplegic cerebral palsy, and a life expectancy that requires 24 hour care.
The Life Care Plan projects every cost across the child’s full life expectancy: physical therapy, occupational therapy, speech therapy, and cognitive rehabilitation with schedules that evolve as the child grows. Anticonvulsant medication management. Adaptive equipment from infant positioning systems through adult power wheelchairs. Home modifications, accessible transportation, specialized education, and vocational support. Attendant care at the level the child’s functional deficits demand. A forensic economist calculates the income the child would have earned across a working career absent the injury. The total is built from documented need, not from sympathy.
For the mother, damages may include hemorrhage requiring transfusion, emergency hysterectomy following uterine rupture, prolonged hospitalization, post-traumatic stress related to the delivery experience, and the psychological impact of watching a child live with an injury that a faster response would have prevented.
How the Defense Turns the Fetal Monitoring Strip Into a Weapon Against You
The hospital’s defense expert will take the same fetal monitoring strip your expert reads as non reassuring and highlight every 30 second segment where the heart rate returned to baseline. They will testify that the overall tracing was “Category II and reassuring” and that “reasonable clinicians can disagree” about when to proceed to cesarean. Attorney Jorge L. Flores watched defense experts build this narrative during the years he spent at a Miami insurance defense firm. He sat in mock trials where defense obstetricians were coached to use the word “reassuring” for tracings that any plaintiff’s perinatologist would call non-reassuring.
The counter to this defense is not another expert opinion in the abstract. It is the timeline. If the strip showed recurrent late decelerations for 90 minutes and no intrauterine resuscitation measures were documented, the defense cannot argue the team was “managing appropriately” because the chart does not reflect any management at all. If Pitocin was increased at the same time the strip was deteriorating, the medication administration record contradicts the claim that the team was responding to the pattern. Jorge Flores builds every delayed C-section case to make the strip and the chart speak for themselves, because a jury that sees the timeline does not need to choose between competing experts. The documents choose for them.
The Strip Was Showing Distress. The Baby Was Still Inside. Every Minute Between Recognition and Delivery Is Documented.
The fetal monitoring record, the nursing notes, the operative report, and the anesthesia log reconstruct the timeline from the first concerning pattern to the moment of birth. If the minutes were lost, the records prove where.
(305) 598-2221
FREQUENTLY ASKED QUESTIONS
What counts as a delayed C-section?+
A delayed C-section is not defined by a fixed number of minutes. It is defined by the relationship between the clinical picture and the timing of the delivery. If the fetal heart rate tracing showed a pattern that required immediate delivery and the team did not move to the operating room for another hour, the delay is measured against what a competent obstetric team would have done in the same clinical situation. The standard is not a clock. It is the strip.
Is every emergency C-section delay malpractice?+
No. Some delays are caused by factors beyond the team’s control, and some clinical situations involve genuine ambiguity about when to intervene. A delay becomes malpractice when the fetal monitoring strip showed a pattern that a reasonably competent obstetrician would have recognized as requiring delivery, and the team waited beyond the timeframe the clinical urgency demanded. The distinction between acceptable management and negligent delay requires expert analysis of the strip, the clinical context, and the response timeline.
How fast should doctors act when the fetal monitor shows distress?+
Many hospitals use a 30 minute target from decision to incision for emergent cesareans. But for crash scenarios involving sustained bradycardia, complete abruption, or uterine rupture, 30 minutes may be too long. The true benchmark is what a competent obstetric team at a similarly equipped Miami hospital could and should have achieved given the severity of the strip and the clinical emergency. Our experts calculate this based on the specific scenario, not a one-size-fits-all number.
How do you prove the delay caused the brain injury and not the pregnancy itself?+
We correlate the fetal monitoring timeline with the neonatal outcome. If the strip was reassuring for most of the labor and deteriorated in a specific, identifiable window, and the baby was born with low Apgar scores, required resuscitation, and developed HIE or seizures, the temporal relationship between the deterioration and the injury is the foundation of causation. Our maternal-fetal medicine specialists and pediatric neuroradiologists work together to demonstrate that the pattern of brain injury on the MRI is consistent with the timing and duration of the oxygen deprivation documented on the strip.
How long do I have to file a delayed C-section case in Miami?+
In many Florida birth injury cases, the limitations period for a minor does not begin to run until around the child’s eighth birthday, though specific deadlines can depend on the facts and statutes in effect at the time of the injury. However, the fetal monitoring strips, the labor nursing notes, the operative report, and the anesthesia record are maintained on the hospital’s retention schedule and can be purged. Contacting us early allows us to issue statutory preservation demands before the strongest evidence is gone.
What does it cost to hire a lawyer for a delayed C-section case?+
Our firm absorbs the full financial burden of the case. The fetal monitoring strip analysis, the maternal-fetal medicine expert review, the pediatric neuroradiology consultation, the Life Care Plan, and the forensic economics report are all funded by us. We collect a fee only when compensation is recovered for your family. If the case does not produce a recovery, the investment was entirely ours.
CONTACT US FOR A FREE CASE REVIEW
If your child suffered a brain injury following a delayed cesarean delivery at a Miami hospital, the Law Offices of Jorge L. Flores, P.A., will review the fetal monitoring strips, the labor records, and the operative timeline at no charge. We reconstruct the minutes between the first non reassuring pattern and the delivery and tell you whether the evidence supports a claim. That conversation costs nothing and commits you to nothing.
Free Case Review. No Cost Unless We Recover Compensation.
We fund the strip analysis, the expert consultations, and the full investigation. Our fee is contingent on the result.
(305) 598-2221
Related: Birth Injuries · Neonatal Seizures · Umbilical Cord Prolapse · Periventricular Leukomalacia (PVL) · Medical Malpractice