

Reviewed by Jorge L. Flores, Esq. · Law Offices of Jorge L. Flores, P.A. · Miami, Florida · Last Updated: March 2026
After hours in a crowded waiting room, you were briefly evaluated, told the symptoms were nothing to worry about, and sent home. Hours later, a frantic hospital readmission revealed a massive stroke, a ruptured appendix, or raging sepsis; entirely present, yet completely missed, during that initial visit.
An exhaustive systematic review published by the Agency for Healthcare Research and Quality (AHRQ) estimated that 1 in 18 emergency department patients receives an incorrect diagnosis; roughly 7.4 million misdiagnosed patients every single year. The data further indicates that 72% of all ER diagnostic errors resulting in serious harm involve the “Big Three” disease categories: vascular events, infections, and cancers. At the Law Offices of Jorge L. Flores, P.A., we represent patients and families throughout the entire State of Florida who have suffered devastating, preventable harm because an emergency room failed at its most fundamental obligation.
WERE YOU SENT HOME FROM THE ER AND THEN RUSHED BACK
If you were discharged from a Florida emergency room and had to return within 72 hours with a condition that was present during the first visit, the “bounce back” is oftentimes the first indicator of a catastrophic diagnostic failure. Seek corrective care at a different hospital system immediately. Request the complete, unedited medical chart from the first ER visit; specify that you require all nursing notes, triage assessments, laboratory results, and the electronic audit trail showing when documents were viewed or altered. Preserve every discharge document; instructions dictating a benign diagnosis serve as powerful evidence. Do not provide a recorded statement to the hospital’s risk management department. An unscheduled return within 72 hours triggers elevated scrutiny by quality review boards; and it should trigger the same scrutiny from your legal team.
1 in 18 ER patients misdiagnosed
7.4 million annual misdiagnoses
72% involve the “Big Three”
THE MISDIAGNOSES THAT KILL
Emergency room diagnostic errors are frequently the result of physician cognitive bias converging with the atypical presentation of life threatening diseases. Identifying these clinical patterns is imperative for proving where the standard of care was breached.
Heart Attacks in Women
Women under 55 are seven times more likely to be sent home without cardiac testing. Women frequently present with “atypical” symptoms; shortness of breath, fatigue, nausea, or jaw and back pain instead of classic chest pressure. In a fast paced ER, these are misattributed to anxiety or acid reflux. When an electrocardiogram is misread or a serial troponin test is omitted, the patient is discharged only to suffer irreversible heart failure or fatal cardiac arrest.
Stroke and Racial Bias
Clot busting tPA is only effective within a narrow window of a few hours. Younger patients with dizziness or mild weakness are frequently misdiagnosed with migraines or vertigo. Minority patients are 20% to 30% more likely to be misdiagnosed; implicit biases lead providers to attribute slurred speech or altered mental status to intoxication or baseline dementia rather than ordering a STAT non contrast CT scan.
The Deadly Mimics: Aortic Dissection and Pulmonary Embolism
Aortic dissection carries 50% mortality at 48 hours if untreated; ER physicians miss it in 15% to 43% of initial visits. Pulmonary embolism is missed when providers misapply the Wells Criteria or PERC Rule. A critical nuance oftentimes missed: a triage tachycardia that normalizes by bedside assessment should still count when calculating the Wells score; ignoring this initial vital sign leads to deadly false negatives.
Appendicitis, Sepsis, and Ectopic Pregnancy
One in three appendicitis patients lacks classic symptoms; frequently misdiagnosed through “premature closure,” where the provider stops investigating once a benign label is attached. Early sepsis signs are routinely dismissed as a viral syndrome; less severe presentations actually increase the risk. Nearly half of ectopic pregnancies are missed during the first physician visit.
WHEN THE SYSTEM ITSELF FAILS
Triage Failures
A study of 5.3 million encounters found mistriage in one third of all patients. Critically ill patients assigned low acuity scores are left unmonitored while heart attacks, internal bleeding, or sepsis progress in the waiting room.
The “Dual Bottleneck”
139.8 million annual ER visits; inpatient capacity has not kept pace. Admitted patients board on ER gurneys; 40% wait 4+ hours during peak months. Newly arriving critical patients cannot be evaluated because ER beds are consumed.
Handoff Failures
I PASS protocols cut handoff errors from 0.42 to 0.06 per encounter. Without them, outgoing physicians’ orders are lost; incoming doctors discharge patients before critical troponin results return.
What This Means for Patients
If you were sent home from the ER and had to come back within hours or days with a condition that should have been caught the first time, the question is not whether the ER doctor was “doing their best.” The question is whether the system around them was set up to fail; and whether the hospital is liable for the triage errors, the overcrowding, and the handoff breakdowns that allowed a life threatening diagnosis to walk out the door.
FLORIDA’S ER LEGAL FRAMEWORK
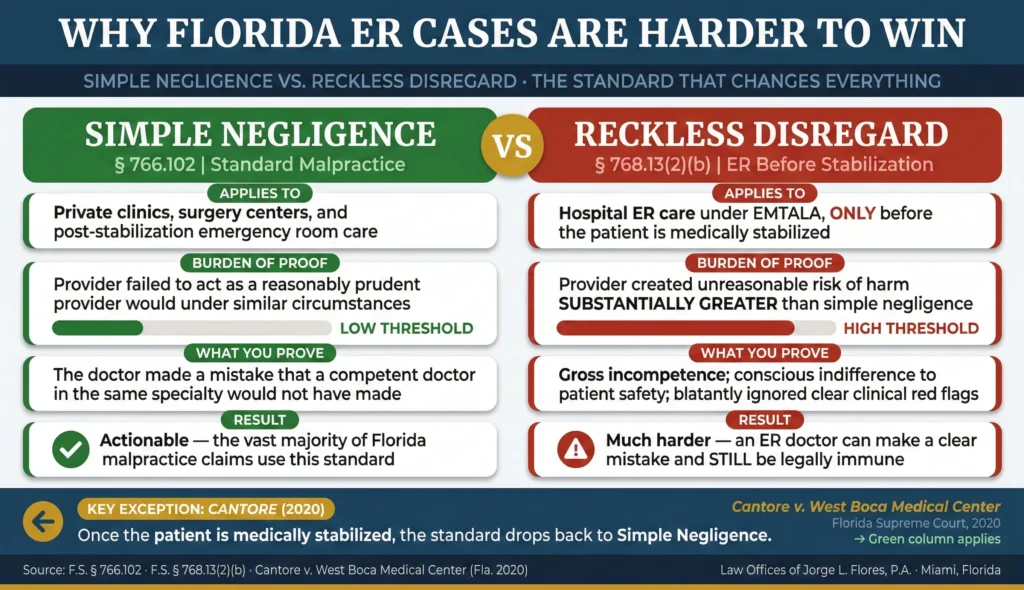
The “Reckless Disregard” Standard
Under standard Florida malpractice law (Section 766.102), a plaintiff proves “simple negligence.” Under Section 768.13(2)(b), when care is provided in a hospital emergency department pursuant to EMTALA, the standard elevates to “reckless disregard”; conduct the provider knew or should have known created an unreasonable risk “substantially greater than that which is necessary to make the conduct negligent.” An ER physician can make a clear diagnostic mistake and still be immune. This elevated standard only applies before stabilization. Once stabilized, simple negligence applies. Per Cantore, treating a non emergent issue in the ER does not trigger the protection.
Same Specialty Expert Witness Requirement
Section 766.102(9) restricts expert testimony: only a physician with “substantial professional experience” in a hospital emergency department within the preceding five years may testify against an ER provider. A board certified cardiologist cannot testify that an ER physician missed a heart attack. This narrows the expert pool significantly and demands careful strategy. For the full pre suit process including the mandatory 90 day screening period, see our pre suit requirements guide.
Sovereign Immunity at Government Hospitals
Tampa General, Jackson Memorial, UF Health Shands, Broward Health; all government owned. Section 768.28 caps damages at $200,000 per person / $300,000 per incident; encompassing all damages combined. Exceeding the caps requires a legislative “Claims Bill” passed by both chambers; a multi year political process.
APPARENT AGENCY: WHO ACTUALLY PAYS
The vast majority of Florida hospitals outsource emergency room physician staffing to corporations like TeamHealth or Envision Healthcare; the attending physicians are technically independent contractors. Florida appellate courts have used the Apparent Agency Doctrine to pierce this shield. If the hospital provided the scrubs, badges, and consent forms, and you reasonably believed the doctor was a hospital employee, the hospital is liable. When a patient arrives in a dire emergency, there is no realistic opportunity to select a specific physician; and if admission forms fail to disclose the independent contractor relationship, courts find apparent agency exists.
Stewart v. Tampa General Hospital (2025): A Hillsborough County jury awarded $70.8 million after an APRN missed clear signs of cerebral blood clots at the Brandon Healthplex. The APRN was employed by InPhyNet (a TeamHealth subsidiary), yet the jury found apparent agency made Tampa General Hospital liable for the full verdict.
EMTALA: THE FEDERAL RIGHT MOST PATIENTS DO NOT KNOW THEY HAVE
Any hospital receiving Medicare funding must (1) provide an “appropriate medical screening examination” to any individual presenting to the emergency room, without delaying for insurance verification, and (2) stabilize any diagnosed emergency condition or arrange a safe transfer. Violations expose the hospital to civil penalties of up to $129,233 per violation and a private cause of action in federal court. The Law Offices of Jorge L. Flores, P.A., has pursued claims including improper screening delays, discriminatory triage, and constructive denial of care.
It is significant to note that EMTALA governs the process of screening, not the accuracy of the diagnosis. EMTALA violations occur when the hospital deviates from its own procedures, discriminates based on payment status, or fails to stabilize a known condition. When extreme overcrowding causes a patient to “Leave Without Being Seen” (LWBS); particularly if staff subtly suggested the patient leave due to lack of insurance; a claim for “constructive denial” of a medical screening may exist.
If an ER diagnostic failure has caused catastrophic harm to you or a loved one, contact the Law Offices of Jorge L. Flores, P.A. for a confidential consultation.
Inside Advantage
Attorney Flores is a former insurance defense attorney who is cognizant of the precise strategies defense counsel deploys in ER cases; the “hindsight bias” defense, the reckless disregard shield, sovereign immunity caps, and the corporate shell game of independent contractor staffing agencies. At the Law Offices of Jorge L. Flores, P.A., we use that institutional knowledge to anticipate and dismantle every defense before it is raised.
The ER was supposed to save your life. Instead, it sent you home to die. If you or a loved one was misdiagnosed in a Florida emergency room, the experienced Law Offices of Jorge L. Flores, P.A., can help.
From our offices in Miami, Florida, we navigate the elevated reckless disregard standard, retain ER specific expert witnesses, investigate the apparent agency chain, and pursue every theory of liability available under Florida law. We handle ER malpractice cases on a contingency basis; you pay nothing unless we recover for you.
P.S. The hospital that sent you home has already documented its version of events. Their risk management team has reviewed the chart, interviewed the attending physician, and begun constructing a defense designed to characterize your misdiagnosis as a “reasonable clinical judgment” under the reckless disregard standard. At the Law Offices of Jorge L. Flores, P.A., we move with the same urgency on your behalf; because the triage records, the nursing notes, and the EHR audit trail that prove exactly what was missed are the evidence that defense teams work hardest to reframe.
Related: Medical Malpractice · Hospital Infections · Premature Discharge · Who Can Be Held Responsible · Failure to Treat