

Reviewed by Jorge L. Flores, Esq. · Law Offices of Jorge L. Flores, P.A. · Miami, Florida · Last Updated: March 2026
They told you to count backward from ten. You remember seven. Then you remember the sound of the surgeon’s voice, the pressure of instruments inside your body, and the paralyzing realization that you could not scream.
The administration of anesthesia is an intricate, highly volatile balance of pharmacology, continuous physiological monitoring, and clinical vigilance. When the standard of care is breached, the consequences are frequently instantaneous and catastrophic; profound anoxic brain injuries, severe cardiovascular collapse, unexpected mortality, and psychological trauma that can haunt a patient for decades. At the Law Offices of Jorge L. Flores, P.A., we represent patients and families throughout the entire State of Florida who have suffered devastating harm because an anesthesia provider failed at one of the most unforgiving disciplines in all of medicine.
IF YOU EXPERIENCED ANESTHESIA AWARENESS OR AN UNEXPLAINED POST SURGICAL INJURY
Request the complete, unedited anesthesia record immediately. This includes the electronic anesthesia data log, the pre operative assessment, the post operative PACU notes, and all pharmacy dispensing records for drugs drawn from the anesthesia cart. These records are your property under federal law.
If you experienced intraoperative awareness, document your experience in writing as soon as possible; every sound, voice, sensation, and detail you remember while the memory is fresh. This contemporaneous account will be critical evidence if you develop PTSD symptoms weeks or months later.
Do not accept the hospital’s explanation that you were “dreaming” or “confused.” Awareness patients routinely report specific, verifiable details from the operating room that can be corroborated against the operative report. Contact an attorney before accepting any characterization of your experience from the facility that harmed you.
ANESTHESIA AWARENESS: THE SILENT NIGHTMARE
Among the most profoundly traumatic events a patient can endure within a healthcare setting is unintended intraoperative awareness. This phenomenon occurs when general anesthesia fails to render a patient completely unconscious, but the neuromuscular blocking agents; potent paralytics such as succinylcholine or rocuronium; successfully maintain total physical paralysis. The patient cannot move, cannot speak, their eyes are typically taped shut, and they cannot signal to the surgical team that they are awake and experiencing agonizing pain.
56.3%
Of Awareness Patients Develop PTSD
17.9 Yrs
Mean Duration of PTSD Symptoms
0%
PTSD Rate Under Proper Anesthesia
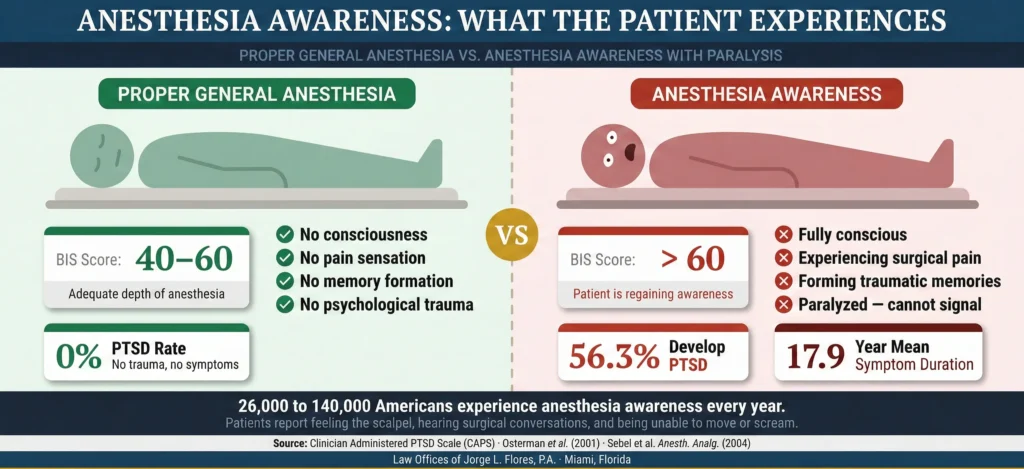
Extensive clinical data indicates that anesthesia awareness occurs in approximately 1 to 2 cases per 1,000 patients receiving general anesthesia; rising to 0.4% in obstetric surgeries, 1.1% to 1.5% in cardiac surgeries, and 0.8% to 1.2% in pediatric patients. Translated to national surgical volumes, this results in an estimated 26,000 to 140,000 cases every single year. Survivors suffer from a constellation of debilitating symptoms, including chronic insomnia, hyperarousal, intrusive night terrors, flashbacks, and an extreme, phobic fear of any future medical care.
THE BIS MONITOR CONTROVERSY
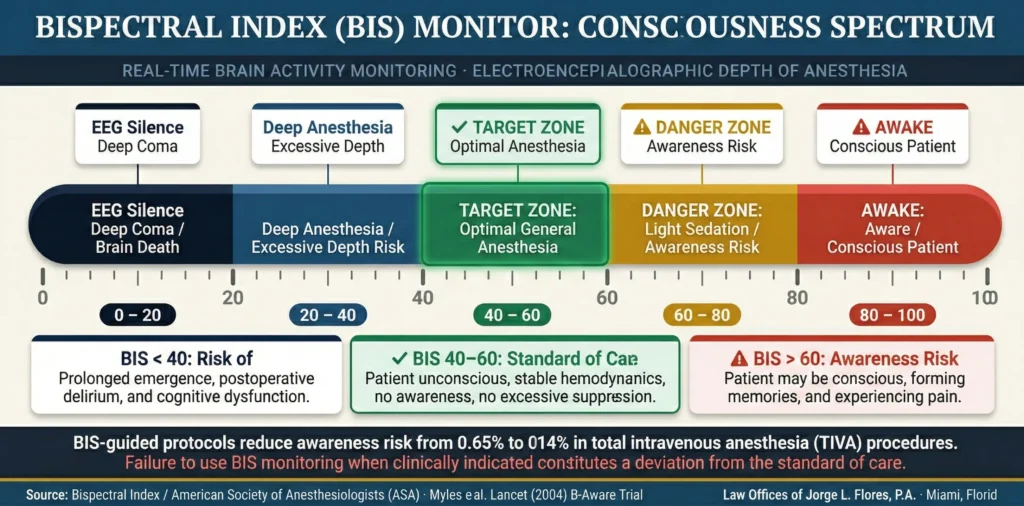
The Bispectral Index (BIS) monitor utilizes sophisticated electroencephalogram (EEG) technology to non invasively measure the electrical activity of a patient’s cerebral cortex, generating a dimensionless score between 0 and 100. A score of 90 to 100 indicates a fully awake patient; a score between 40 and 60 represents the optimal targeted depth of general anesthesia; and a flatline score of 0 indicates complete suppression of cortical activity. Despite the profound trauma associated with anesthesia awareness, the American Society of Anesthesiologists (ASA) has not universally mandated BIS monitoring as a baseline standard for every surgical procedure.
When Failure to Use the BIS Monitor Becomes Negligence
Large scale randomized controlled trials have demonstrated that BIS guided protocols can reduce the risk of awareness from 0.65% to 0.14% in propofol based Total Intravenous Anesthesia (TIVA). When an anesthesiologist is fully aware of a patient’s heightened risk profile; such as a documented history of substance abuse, severe hemodynamic instability, or a prior episode of awareness; possesses BIS monitoring technology within the facility, but actively chooses not to deploy it, the foundation for a negligence claim strengthens considerably.
CATEGORIES OF ANESTHESIA ERRORS
Anesthesia malpractice is not limited to intraoperative awareness. The scope of potential negligence encompasses every phase of perioperative care, and the Law Offices of Jorge L. Flores, P.A., is cognizant that each specific error category produces distinct, devastating physiological injuries that require highly specialized expert testimony to prove in a Florida courtroom.
Dosing Errors
Excessive anesthesia can lead to immediate cardiovascular collapse, respiratory depression, severe hypotension, and permanent anoxic brain damage. Insufficient doses directly cause the anesthesia awareness and ensuing PTSD. Every dosing calculation must account for the patient’s age, weight, lean body mass, and highly specific metabolic factors.
Airway Management Failures
The human brain can only tolerate a lack of oxygen for a matter of minutes before irreversible cellular death occurs. If an anesthesiologist becomes distracted, ignores critical monitor alarms, or fails to recognize that an endotracheal tube has become dislodged, the patient will suffer devastating hypoxic brain injury; frequently resulting in a permanent vegetative state or wrongful death. Any patient presenting with a Mallampati Class III or IV airway must have a specific, documented difficult airway plan and emergency equipment immediately available before anesthesia is induced.
Aspiration of Gastric Contents
General anesthesia paralyzes the protective reflexes of the airway. If the anesthesiologist fails to confirm strict adherence to NPO fasting guidelines, or fails to perform a rapid sequence induction in a high risk patient, acidic stomach contents can be regurgitated and inhaled directly into the lungs. This causes aspiration pneumonitis; a severe, life threatening chemical burn and infection of the lung tissue that frequently leads to acute respiratory distress syndrome (ARDS) and death.
Improper Positioning and Nerve Damage
While unconscious and paralyzed, the patient loses all ability to protect their joints and nerves. The anesthesia team has a non delegable duty to properly position and pad the patient throughout the procedure. Failing to pad bony prominences or allowing a limb to hang off the table can result in permanent damage to the brachial plexus or ulnar nerve compression, leaving the patient with permanent numbness, chronic pain, or total loss of motor function.
Medication Swap Errors
Pharmaceutical manufacturers oftentimes utilize strikingly similar vial sizes, cap colors, and label designs for drugs with drastically different mechanisms of action. When bupivacaine (a spinal anesthetic) is accidentally swapped with tranexamic acid (an antifibrinolytic); both often in nearly identical 10ml vials with yellow caps; injection into the spinal canal causes catastrophic neurotoxicity, intractable seizures, and frequently death. The standard of care strictly dictates that the provider must read the label of every medication drawn before injection.
What This Means for Patients
You were unconscious when the error occurred. You have no memory of what went wrong. That is precisely why the electronic anesthesia data log; which records every drug administered, every vital sign reading, and every alarm that was triggered or silenced, second by second; is the single most important piece of evidence in your case. We know how to obtain it, how to read it, and how to use it to prove exactly what happened while you were unable to protect yourself.
Malignant Hyperthermia: The Preventable Genetic Crisis
Malignant Hyperthermia (MH) is a rare, exceptionally severe pharmacogenetic disorder triggered by volatile anesthetic gases or succinylcholine. In genetically susceptible individuals, exposure triggers a massive, uncontrolled release of intracellular calcium, inducing a hypermetabolic state with rapidly spiking body temperature, severe acidosis, and cardiac arrest. The only effective antidote is intravenous Dantrolene; clinical data shows that a 50 minute delay in administration results in a 100% complication or mortality rate. Under the Florida Administrative Code (Rules 64B8-9.009 and 64B15-14.007), any office surgery center in Florida that utilizes triggering agents is legally required to stock at least 720 mg of Dantrolene on site at all times. If a patient dies from an MH crisis and discovery reveals the facility failed to stock this legally mandated supply, establishing gross negligence is generally straightforward.
Post Operative Cognitive Dysfunction (POCD) is a deeply underserved claim in medical malpractice litigation. This neurological syndrome is characterized by a persistent decline in long term memory, executive function, and information processing following surgery and general anesthesia. Approximately 40% of patients over age 60 exhibit clear signs of POCD at hospital discharge, and 10% to 12% continue to suffer significant cognitive impairment three months after the operation. POCD is frequently misattributed to natural aging or dementia, but the pathogenesis is intensely tied to the anesthesiologist’s intraoperative management; specifically, extended periods of hypotension or inadequate cerebral oxygenation. When the electronic data logs reveal blood pressure was permitted to remain dangerously low without aggressive pharmacological intervention, a viable negligence claim may exist.
RECOVERY ROOM FAILURES
The anesthesiologist’s duty of care does not terminate when the surgeon closes the final incision. The immediate post operative period, managed in the Post Anesthesia Care Unit (PACU), is a highly volatile phase where the patient is actively metabolizing heavy narcotics, paralytics, and hypnotic agents. A staggering 43% of anesthesia malpractice claims involve severe communication failures, with the vast majority occurring during the critical transfer of care from the anesthesia team to the PACU nursing staff.
Common PACU errors include premature extubation before residual paralytic agents have been adequately reversed, failure to recognize a gradually dropping oxygen saturation in a heavily sedated patient, and improper handoff where the anesthesiologist fails to inform PACU nurses of specific intraoperative complications or narcotic dosages administered; leaving recovery nurses entirely unprepared for sudden, predictable physiological deterioration.
If you or a loved one suffered an anesthesia related injury, contact the Law Offices of Jorge L. Flores, P.A. for a confidential consultation before critical evidence is lost.
CRNA VS. ANESTHESIOLOGIST LIABILITY
One of the most legally complex aspects of pursuing an anesthesia malpractice claim is identifying who was actually responsible for the patient’s care. Most patients assume a physician anesthesiologist personally administered their drugs for the entire procedure. In modern reality, anesthesia care heavily relies on Certified Registered Nurse Anesthetists (CRNAs), and the liability frameworks governing their practice in Florida are undergoing unprecedented legislative changes.
The 2025 Paradigm Shift: HB 649 and Autonomous CRNA Practice
Effective July 1, 2025, Florida House Bill 649 authorizes completely autonomous practice for CRNAs who have completed at least 3,000 hours of physician supervised clinical practice within the previous five years and meet specific continuing education requirements. Autonomous CRNAs in licensed hospitals or ambulatory surgical centers are explicitly exempted from the statutory requirement that anesthesia be administered under physician supervision. For procedures after July 1, 2025, patients may no longer be able to name a supervising anesthesiologist or rely on vicarious liability, because the legal requirement for physician supervision has been severed. The liability will rest squarely on the autonomous CRNA and potentially the facility; making procurement of internal credentialing documents a critical first step in discovery.
Under the historical supervision model, a single physician anesthesiologist may concurrently supervise up to four CRNAs in four separate operating rooms. When a CRNA commits a negligent error under supervision, Florida law allows the patient to pursue claims against both the CRNA and the supervising physician or hospital, based on vicarious liability, respondeat superior, or the “Captain of the Ship” doctrine. Facilities may still require supervisory protocols via internal corporate bylaws even after HB 649, making the analysis of hospital policies imperative in every anesthesia case.
THE FLORIDA IMPACT RULE AND PSYCHOLOGICAL DAMAGES
Securing financial compensation for the trauma of anesthesia awareness is uniquely challenging because the profound injury is oftentimes almost entirely psychological. Florida is one of a shrinking minority of jurisdictions that continues to strictly adhere to the “Impact Rule,” originating from the foundational 1893 Florida Supreme Court decision in International Ocean Telegraph Co. v. Saunders. This rule harshly dictates that a plaintiff cannot recover damages for purely emotional or psychological distress unless that distress was directly caused by a physical impact or resulted in a discernible, verifiable physical injury.
Experienced attorneys navigate around the Impact Rule using established exceptions. Under Zell v. Meek (665 So. 2d 1048), if the patient’s awareness induced PTSD manifests in verifiable physical symptoms; such as stress induced hypertension, severe weight loss, or gastrointestinal ulcers; the “discernible physical injury” requirement may be satisfied. Under the “freestanding tort” exception established in Kush v. Lloyd (616 So. 2d 415), if the anesthesiologist’s conduct demonstrated reckless disregard for patient safety, the Impact Rule can be bypassed entirely. Additionally, even minor physical complications documented in the surgical record; such as a chipped tooth from intubation or a corneal abrasion; can be leveraged as the requisite physical impact to unlock the full spectrum of recoverable damages.
Why the Impact Rule Matters for Awareness Victims
If you experienced anesthesia awareness and are suffering from PTSD, nightmares, and the inability to undergo future medical procedures, your legal team must map the strategy around the Impact Rule before the complaint is even drafted. A chipped tooth or a bruise from positioning may seem trivial compared to years of psychological torment; but in a Florida courtroom, that minor physical impact is the legal key that unlocks your right to recover for everything else.
Under Florida Statute Section 766.103, the duty to obtain informed consent is completely non delegable. Florida courts have consistently held that the surgeon cannot obtain informed consent on behalf of the anesthesiologist. The anesthesiologist has an independent legal duty to discuss the unique risks of the anesthetic plan. If they negligently rely on the surgeon’s generic consent form and fail to conduct a separate, anesthesia specific risk disclosure, they can be held directly liable; regardless of how flawlessly they performed during the procedure.
Effective January 1, 2025, Florida Statutes Section 766.118 imposes a $750,000 cap on non economic damages per claimant in medical negligence cases; with a $1.5 million exception for catastrophic injuries such as permanent vegetative state or irreversible paralysis. Economic damages remain completely uncapped. The 2025 caps represent a particularly severe blow to anesthesia awareness victims, whose injuries are predominantly psychological. This makes it imperative that your legal team aggressively quantify the economic components of your PTSD; including the cost of years of psychiatric treatment, psychotropic medication, lost employment, and the need for ongoing therapeutic care. For a full breakdown of damage categories, see our types of compensation guide. Florida’s mandatory pre suit investigation requires retaining a board certified anesthesiologist to review the case before any lawsuit can be filed.
Inside Advantage
Attorney Flores worked as an attorney for a top rated insurance defense firm in Miami, where he learned first hand how hospitals and their insurers defend anesthesia error claims. He knows how defense teams aggressively deploy the Florida Impact Rule to bar psychological damage claims, how they invoke HB 649 to sever supervisory liability chains, and how they routinely characterize preventable errors as “known complications” documented in the patient’s signed consent form. That experience is why every anesthesia case we build is constructed not just to prove the error, but to preemptively navigate the unique legal obstacles that make anesthesia claims among the most technically demanding in all of medical malpractice.
“Anesthesia cases are among the most forensically demanding claims in all of medical malpractice. The anesthesia record is a minute by minute data log of every drug administered, every vital sign recorded, and every alarm that was triggered or silenced. As a former insurance defense attorney, I know that hospitals will attempt to characterize a preventable overdose as an ‘idiosyncratic reaction’ or dismiss awareness as ‘extremely rare.’ We do not allow that narrative to stand.”
Jorge L. Flores, Esq.
You were supposed to wake up safe. You did not. If you or a loved one has suffered anoxic brain damage, intraoperative awareness, a devastating medication swap, or any other catastrophic injury caused by an anesthesia provider, the experienced Law Offices of Jorge L. Flores, P.A., can help.
From our offices in Miami, Florida, we subpoena the raw electronic anesthesia data, retain board certified anesthesiologists as expert witnesses, reconstruct every second of the perioperative timeline, and navigate the unique legal obstacles; including the Impact Rule and HB 649; that make these cases among the most complex in medical malpractice. We handle anesthesia error cases on a contingency basis; you pay nothing unless we recover for you.
P.S. Patients who have experienced anesthesia awareness oftentimes struggle to be believed; by their families, by subsequent physicians, and even by themselves. The terror of being awake and paralyzed during surgery is so incomprehensible to those who have not experienced it that victims are frequently told they must have been “dreaming” or “confused.” You were not dreaming. What happened to you was real, it was preventable, and the Law Offices of Jorge L. Flores, P.A., is here to prove it.
Related: Medical Malpractice · Surgical Errors · Who Can Be Held Responsible · Informed Consent · Types of Compensation