

Reviewed by Jorge L. Flores, Esq. · Law Offices of Jorge L. Flores, P.A. · Miami, Florida · Last Updated: April 2026
Are You in a Hospital Right Now and Being Told to Leave?
1. Say this out loud to your nurse: “I do not feel safe to go home. Please document my objection in the medical record right now.”
2. If you are on Medicare: Find the paper titled “An Important Message from Medicare About Your Rights.” Call the phone number on it before noon today. This legally stops the hospital from sending you home while your case is reviewed.
3. Ask for the Patient Advocate. Every hospital has one. Tell them you are filing a formal grievance about an unsafe discharge.
4. Do NOT sign an “Against Medical Advice” form. Staff may tell you that your insurance will not pay if you refuse to leave. That is not true. You are not refusing treatment; you are asking for more of it.
5. Ask the nurse to read your vital signs out loud. If your heart rate, blood pressure, or oxygen level is abnormal, say: “My vitals are not stable. I need a doctor to come back and evaluate me before I leave.” If you have already been sent home and are getting worse, call 911 first, then contact our team.
The doctor signed the discharge order. Hours later, you were back in the emergency room; seizing, hemorrhaging, or fighting for your life. The hospital will call it an unfortunate complication. The data tells a different story.
The Law Offices of Jorge L. Flores, P.A., in Miami, Florida, understands that premature hospital discharge is rarely an isolated error in clinical judgment; it is the predictable byproduct of a healthcare system engineered to prioritize bed availability, throughput metrics, and financial reimbursement over individualized patient safety. We are committed to providing aggressive, meticulous legal representation to patients and families throughout the State of Florida who have suffered catastrophic harm because a hospital sent them home before they were medically stable.
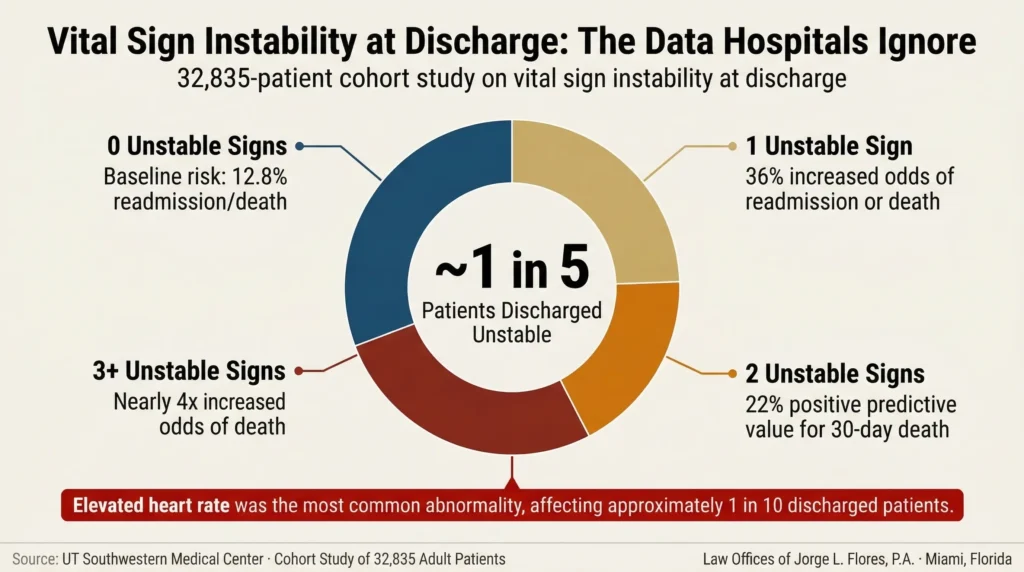
1 in 5
Hospital Patients Discharged With Unstable Vital Signs
4x
Increased Odds of Death With 3+ Unstable Signs
3%
Maximum CMS Medicare Penalty for Excessive Readmissions
Sources: UT Southwestern Medical Center · 32,835 Patient Cohort Study · CMS Hospital Readmissions Reduction Program
WHY HOSPITALS DISCHARGE PATIENTS TOO EARLY
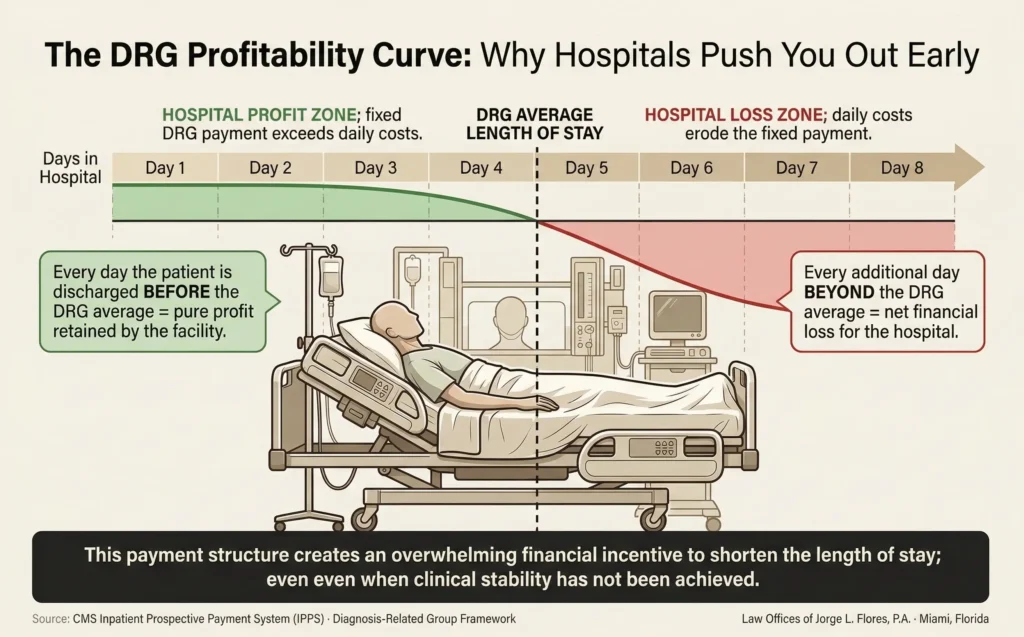
Premature discharge is not an accident. It is the predictable consequence of a reimbursement system that rewards hospitals for shorter stays and penalizes them for longer ones. Under the federal Diagnosis Related Group (DRG) payment system, a hospital receives a predetermined, flat rate payment based solely on the patient’s admission diagnosis; regardless of the actual costs incurred or the number of days the patient remains in the bed.
DRG Profitability Pressure
Attending physicians receive regular alerts from hospital case management departments detailing the “expected length of stay” for their patients; creating an administrative drumbeat to authorize discharges the moment a patient meets the bare minimum criteria for clinical stability.
ER Boarding and Bed Pressure
When no inpatient beds are available, patients stack up in the emergency department. Target discharge times of 11:00 AM are imposed on clinical staff to clear rooms before the afternoon surge of surgical recoveries and new ED admissions.
Utilization Review Denials
Insurance companies employ remote utilization review departments that authorize or deny payment for hospital days. When an insurer issues a coverage denial, patients are oftentimes told “your insurance will no longer cover your stay”; a statement that implies the patient has no choice, when in fact the hospital’s medical duty does not evaporate because an insurer refuses to pay.
The Observation Status Trap
It is significant to note that if a patient is placed in “observation status,” they are legally classified as an outpatient; even while physically lying in a hospital bed receiving round the clock nursing care. Medicare covers observation under Part B rather than Part A, subjecting the patient to higher costs. Critically, observation time does not count toward the three consecutive inpatient days required before Medicare will cover transfer to a skilled nursing facility. Under Florida Statute Section 395.301 and the federal NOTICE Act, hospitals must immediately notify patients of observation status.
THE SIX CLINICAL PATTERNS OF PREMATURE DISCHARGE
| Discharge Pattern | Clinical Mechanism | Key Evidence |
|---|---|---|
| Before Diagnostic Workup Complete | Patient sent home while blood cultures, troponin series, or imaging results are still pending. | Electronic medical record showing “results pending” at the exact time the discharge order was signed. |
| Before Medical Stability | Patient discharged with documented abnormal vital signs; elevated heart rate, fever, hypoxia, or unstable blood pressure. | Vital sign flowsheets at the exact minute of discharge showing instability. |
| Inadequate Post Discharge Planning | Patient released to a home where they live alone without home health, physical therapy, or the ability to obtain critical medications. | Absence of discharge planning documentation; no home health referral, no pharmacy coordination. |
| Post Surgical Premature Discharge | Patient released before an adequate observation period to monitor for occult bleeding, deep space infections, or anesthesia complications. | Surgical operative report, post anesthesia recovery notes, and timeline proving inadequate observation window. |
| Newborn and Maternal Discharge | Neonate discharged before 48 hours without adequate bilirubin screening. Elevated bilirubin becomes neurotoxic, causing kernicterus; permanent brain damage resulting in cerebral palsy. | Transcutaneous bilirubin readings, nursing notes regarding jaundice, absence of scheduled follow up within 24 hours. |
| Psychiatric Premature Discharge | Patient with active suicidal ideation released from a Baker Act hold without medication stabilization or a 72 hour follow up appointment. | Psychiatric evaluation notes, safety plan documentation (or absence thereof), medication records. |
What This Means for Patients
If you were sent home from a hospital and had to come back within hours or days with a condition that was already present; or developing; at the time of discharge, the question is not whether the doctor made a “judgment call.” The question is whether the vital signs, lab results, and clinical presentation at the exact minute of discharge showed a patient who was not ready to leave. The electronic medical record timestamps answer that question.
If you or a loved one was discharged and suffered catastrophic harm within hours or days, contact the Law Offices of Jorge L. Flores, P.A. for a free consultation.
YOUR RIGHTS TO FIGHT A PREMATURE DISCHARGE IN REAL TIME
Many patients and families assume that once a doctor signs a discharge order, they have no recourse but to gather their belongings and leave. This is legally inaccurate.
Medicare QIO Appeal — Federal Right to Halt the Discharge
Medicare patients must receive “An Important Message from Medicare About Your Rights” within two days of admission. If the patient believes the discharge is unsafe, they must contact the BFCC QIO by noon of the scheduled discharge day. The hospital is then legally prohibited from discharging the patient or billing them while the review is pending.
Demand Documentation of Your Objection
Explicitly tell the attending nurse: “I do not feel medically stable enough to leave. Document my objection to discharge in the electronic medical record right now.” This creates a contemporaneous legal record proving the hospital was on notice.
The “Against Medical Advice” Trap
When a patient refuses to leave because they feel too ill, nursing staff oftentimes present an AMA discharge form and falsely warn that signing it means “your insurance will refuse to pay.” Retrospective studies examining tens of thousands of hospital discharges have repeatedly proven that insurers do not deny claims simply because a patient leaves AMA. The threat is designed to coerce compliance. Patients should firmly refuse to sign and clearly state: “I am not refusing medical advice; I am requesting continued medical treatment because I am unstable.”
WHO IS LIABLE FOR PREMATURE DISCHARGE
Liability for a premature discharge rarely rests on a single set of shoulders.
The Hospitalist
Inpatient care is overwhelmingly managed by hospitalists employed directly by the hospital or a staffing group. The hospitalist who signs the discharge order without fully reconciling conflicting specialist opinions bears primary clinical exposure.
Nursing Staff
Nurses conduct the final assessments before the patient leaves. If a patient is exhibiting unstable vitals at the moment of discharge, the nurse has an independent duty to halt the process, notify the physician, and escalate through the chain of command.
The Hospital (Corporate Negligence)
If systemic throughput policies, DRG driven administrative pressure, or understaffing forced the unsafe discharge, the hospital itself faces direct corporate liability.
The Invisible Defendant: ERISA and the Insurance Shield
The most frustrating aspect of premature discharge litigation is the legal shield protecting the entity that oftentimes forced the discharge; the insurance company. Under the federal Employee Retirement Income Security Act (ERISA), private employer sponsored health insurers are largely immunized from state medical malpractice claims for utilization review coverage decisions. We focus liability on the hospital and physicians; arguing that a doctor’s paramount duty is to the patient’s safety, and capitulating to an insurer’s denial of payment does not legally excuse the physician for abandoning a clinically unstable patient.
THE BARBARA DAWSON CASE: WHEN THROUGHPUT KILLS
In December 2015, Barbara Dawson sought emergency treatment at Calhoun Liberty Hospital in Blountstown, Florida, for severe abdominal pain and shortness of breath. After initial evaluation, staff ordered her discharge. Dawson pleaded that she could not breathe and explicitly refused to leave. Rather than reassessing her worsening respiratory status, the hospital contacted police to have her forcibly removed. An officer handcuffed her and escorted her out. She collapsed in the parking lot. She was pronounced dead approximately 90 minutes later from a massive pulmonary saddle embolism. The Florida Agency for Health Care Administration cited the hospital for 10 egregious deficiencies.
Inside Advantage
Hospitals do not defend premature discharge claims by admitting they needed the bed. They rewrite the narrative. Attorney Flores knows this playbook intimately because he ran it. Before founding this firm, he worked as an attorney for a top rated insurance defense firm in Miami, defending hospitals against exactly these claims. He knows which internal documents to subpoena, which administrative communications to demand in discovery, and precisely where the gap between the clinical record and the economic reality will be widest.
Proving that a premature discharge constitutes medical malpractice requires satisfying strict legal and procedural thresholds under Florida’s Chapter 766 pre suit requirements; including obtaining a verified expert affidavit and serving a formal Notice of Intent triggering a mandatory 90 day investigation period. For the types of damages and fee structure, see the linked guides.
If you or a loved one was discharged from a Florida hospital before achieving medical stability and suffered catastrophic harm as a result, the experienced Law Offices of Jorge L. Flores, P.A., can help.
From our offices in Miami, Florida, we forensically deconstruct the DRG payment timelines, utilization review denial chains, and vital sign flowsheets that prove the discharge was driven by economics rather than clinical readiness. We advance all costs on your behalf. You pay nothing unless we recover compensation.
P.S. The hospital’s risk management team began building its defense the moment you were readmitted. At the Law Offices of Jorge L. Flores, P.A., we move immediately to secure the complete electronic medical record; including the vital sign flowsheets at the exact minute of discharge, the pending lab results the physician never reviewed, the utilization review denial correspondence, and the DRG coding data that reveals the financial pressure behind the decision. Call today; because you deserve an honest answer about whether you have a viable claim.
Related: Medical Malpractice · Hospital Negligence · Nursing Malpractice · Hospital Infections · Wrongful Death