

Reviewed by Jorge L. Flores, Esq. · Law Offices of Jorge L. Flores, P.A. · Miami, Florida · Last Updated: March 2026
You took the medication your doctor prescribed. You trusted it was the right drug, the right dose. It was not.
Patients trust that the medications they receive have been carefully prescribed, accurately dispensed, and safely administered. That trust is the bedrock upon which every clinical encounter is built. Yet preventable medication errors kill between 44,000 and 98,000 Americans in hospitals each year; exceeding the combined annual fatalities from motor vehicle accidents, breast cancer, and AIDS. At the Law Offices of Jorge L. Flores, P.A., we represent individuals and families throughout the entire State of Florida who have suffered catastrophic harm because a healthcare provider failed at the most fundamental act of modern medicine; delivering the right drug, in the right dose, to the right patient, at the right time, through the right route.
IF YOU SUSPECT A MEDICATION ERROR CAUSED YOUR INJURY
Request your complete, unedited medical file immediately. This includes the Medication Administration Record (MAR), the pharmacy dispensing logs, the EHR audit trail showing any override alerts, and all laboratory results ordered before and after the medication was administered. Do not sign any documents from hospital risk management. Any paperwork presented to you in the aftermath of a suspected medication error may contain language that limits your legal rights. If you received the wrong medication at a retail pharmacy, do not return the bottle. It is physical evidence. Photograph the label, the pills, and the receipt, and store them in a safe location. Hospital EHR systems log metadata and override data in real time, but pharmacy dispensing records can be altered or overwritten. Act immediately.
DID THE MEDICATION CAUSE THE HARM
One of the most profound hurdles in medication error litigation is bridging the gap between a patient’s suspicion and objective legal proof. A patient who suffers a catastrophic decline following the administration of a drug oftentimes faces an overwhelming sense of uncertainty: how do I know the medication caused my reaction, rather than my underlying illness? This uncertainty is frequently weaponized by defense attorneys and insurance conglomerates, who will aggressively argue that the harm was an unavoidable complication of the patient’s pre existing comorbidity.
The Critical Legal Distinction
A known side effect becomes the basis for a malpractice claim only if the healthcare provider failed to uphold the reasonable standard of care; for instance, by ignoring a documented allergy, prescribing a contraindicated dosage, or failing to monitor for toxicity. If a patient experiences a known allergic reaction, but their chart clearly indicated this allergy prior to administration, the event shifts from an unfortunate clinical outcome to actionable negligence.
To demonstrate causation effectively, legal teams must construct an impenetrable timeline using specific categories of evidence. Hospital admission and discharge records establish the patient’s baseline health prior to medication administration. Laboratory test results are critical; elevated serum drug levels, sudden spikes in liver enzymes, or dropping glomerular filtration rates provide objective, biochemical proof of an adverse reaction. Florida law requires testimony from highly qualified medical experts; including pharmacologists, toxicologists, or board certified physicians in the defendant’s exact specialty; to explain precisely how the medication error deviated from the prevailing professional standard of care.
THE CHAIN OF CUSTODY: FROM PRESCRIPTION TO PATIENT
A pervasive misconception among patients is that a medication error is an isolated mistake made by a single individual. In reality, the modern hospital and retail pharmacy operate through a highly complex, multi tiered chain of custody where a medication order passes through numerous healthcare professionals, automated dispensing cabinets, and electronic networks before it reaches the patient. An error can originate at any link in this chain, and each link represents a distinct point of liability involving different defendants.
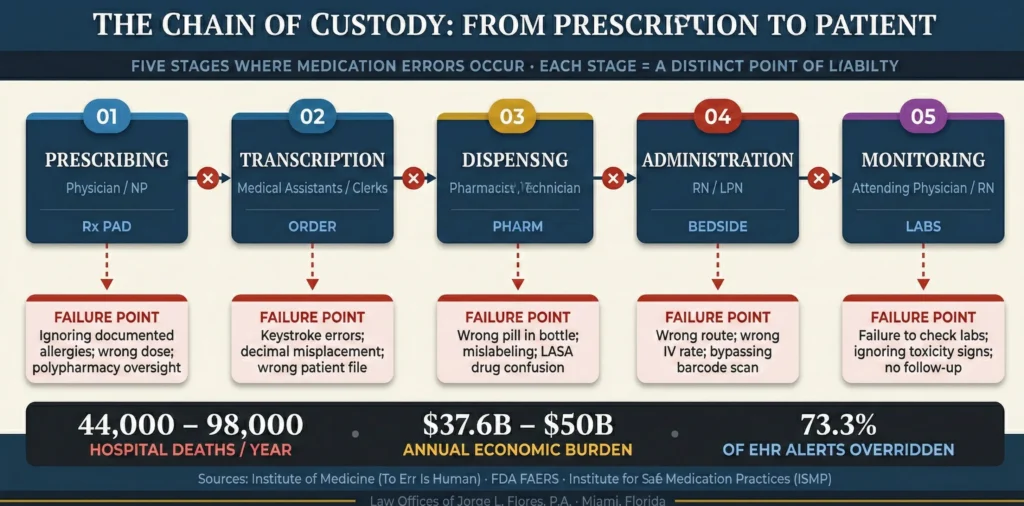
Prescribing Errors
Originate with the physician, nurse practitioner, or physician assistant who selects the pharmaceutical agent. These failures occur when a practitioner specifies an inappropriate dosage or frequency, fails to review a patient’s chart for documented drug allergies, or neglects to check for potentially fatal drug interactions. In the contemporary healthcare environment, prescribing errors are frequently compounded by an over reliance on flawed electronic drop down menus, where a momentary lapse in concentration can result in the selection of a dangerous, look alike medication.
Transcription and Order Entry Errors
Occur when a prescription is inaccurately transmitted into the pharmacy or hospital administration system. While electronic prescribing has mitigated the historical problem of illegible physician handwriting, it has birthed a new category of digital errors; including keystroke mistakes, decimal point misplacements, and the inadvertent selection of the wrong patient file within the Electronic Health Record database. An order entry mistake that transforms a 1.0 mg dose into a 10 mg dose creates a lethally amplified directive that moves silently through the system.
Dispensing Errors
Occur within the physical confines of the pharmacy, where pharmacists and pharmacy technicians fulfill a prescription with the wrong medication, dispense an incorrect dosage strength, or affix inaccurate instructions to the pill bottle. These errors are particularly rampant in high volume retail environments plagued by understaffing, intense corporate pressure to meet fulfillment metrics, and constant interruptions. Dispensing errors also encompass failures of omission, such as a pharmacist failing to conduct a mandatory drug utilization review.
Administration Errors
Statistically the most frequent type of medication mistake resulting in immediate, measurable patient harm. These bedside failures; typically involving registered nurses; include giving a medication via the wrong route, infusing an IV medication at an improperly programmed rate, or administering a drug to the wrong patient entirely. The failure to adhere to institutional safety protocols, such as bypassing bedside barcode medication administration (BCMA) scanning, is frequently cited as gross negligence.
Monitoring Errors
One of the most insidious forms of medication negligence. The duty of care does not vanish once a pill is swallowed or an IV drip is initiated. These failures occur when healthcare providers neglect to order mandatory blood tests to check serum drug levels, fail to assess renal and hepatic function panels to ensure the drug is being safely metabolized, or blatantly ignore the early clinical signs of toxicity. A failure to monitor transforms a safe therapeutic intervention into a lethal overdose over the course of hours or days.
What This Means for Patients
A medication error is rarely one person’s mistake. It is a chain of failures. When your doctor prescribed the wrong drug, the pharmacist should have caught it. When the pharmacist dispensed it anyway, the nurse should have questioned it. When the nurse administered it without checking, the monitoring team should have detected the toxicity. Every link in that chain is a separate defendant. We investigate all of them.
THE “5 RIGHTS” OF MEDICATION ADMINISTRATION
At the absolute core of nursing education, pharmacological training, and hospital protocols is a fundamental safety framework known universally as the “5 Rights” of medication administration. The National Coordinating Council for Medication Error Reporting and Prevention (NCC MERP) explicitly defines a medication error as any preventable event that may cause inappropriate medication use or patient harm while the drug is under the control of the healthcare professional. The failure to verify any single “Right” constitutes per se negligence under the prevailing standard of care.
The 5 Rights Framework
Right Patient: Verify identity using at least two unique identifiers (full name and date of birth) prior to administration.
Right Drug: Confirm that the physical medication selected matches the exact medication ordered. This catches confusion between look alike, sound alike (LASA) drug pairs.
Right Dose: Verify that the mathematical dosage calculation is correct based on the patient’s age, total body weight, and current renal function.
Right Route: Confirm the intended mechanism of delivery. Fatal outcomes routinely occur when medications intended for oral consumption are accidentally injected intravenously.
Right Time: Administer at the correct, scheduled interval. Giving a dose too soon can cause overlapping drug levels resulting in lethal toxicity.
HIGH RISK MEDICATIONS AND CATASTROPHIC OUTCOMES
The Institute for Safe Medication Practices (ISMP) specifically designates certain pharmaceutical classifications as “High Alert Medications”; drugs that bear a significantly heightened risk of causing severe patient harm when used in error.
Anticoagulants
Warfarin · Heparin · Enoxaparin
Massive hemorrhaging · Fatal stroke
Insulin
Humalog · Lantus · Novolog
Hypoglycemic coma · Brain damage
Opioids
Fentanyl · Dilaudid · Oxycodone
Respiratory depression · Cardiac arrest
Chemotherapy
Cyclophosphamide · Vincristine
Organ destruction · Immune collapse
Medication errors are up to three times more likely to occur in pediatric populations, primarily due to complex pharmacokinetics of children whose developing organ systems process drugs differently. The most devastating pediatric mistake is the “10 fold” or “10x” dosing error; a catastrophic event that almost invariably stems from the misplacement of a decimal point during prescribing, transcribing, or pump programming.
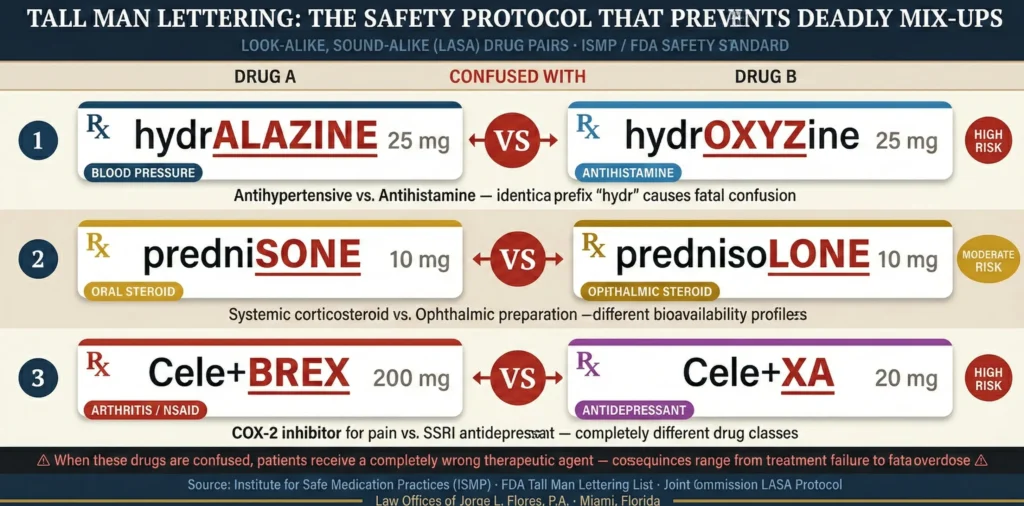
Equally dangerous is the confusion between Look Alike, Sound Alike (LASA) drug pairs. The antihistamine hydroxyzine is frequently confused with the potent blood pressure medication hydralazine; the anticonvulsant levetiracetam is mixed up with the antibiotic levofloxacin; and the arthritis medication Celebrex is frequently dispensed instead of the antidepressant Celexa. The ISMP and the FDA instituted “Tall Man Lettering,” which requires pharmacies and EHR systems to use uppercase, bolded lettering to visually highlight dissimilarities in confusable drug names (for example, differentiating hydrALAZINE from hydrOXYzine). A facility’s failure to implement this protocol is cited as a direct deviation from the prevailing standard of care.
ALERT FATIGUE AND SYSTEMIC NEGLIGENCE
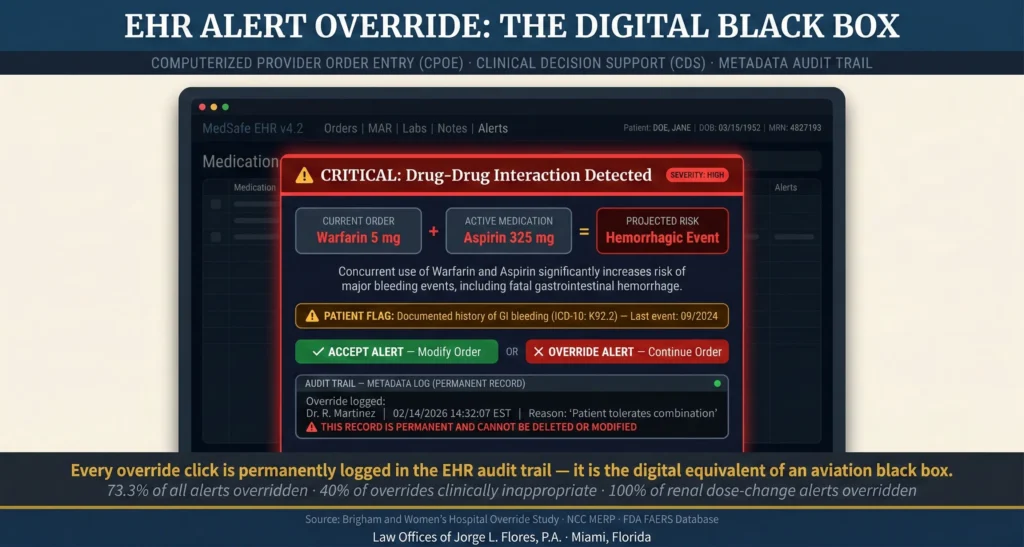
73.3%
Of All Medication Alerts Overridden
40%
Of Overrides Clinically Inappropriate
100%
Renal Dose Change Alerts Overridden
Clinical Decision Support systems are notoriously hyper sensitive, generating thousands of low level, clinically inconsequential warnings. In intensive care units, physiological monitoring systems can generate over two million alerts in a single month; translating to 187 warnings per patient, per day. Physicians become psychologically desensitized, overriding the vast majority of warnings and treating them as digital nuisances rather than safety nets.
Why This Matters for Your Case
When a physician ignores a bright red warning on their computer screen advising them that a newly prescribed drug will fatally interact with a patient’s current medication, that digital click; the “override”; is permanently and irrevocably logged in the metadata audit trail of the EHR system. Through the legal discovery process, securing this digital footprint provides undeniable, time stamped proof of a breach of duty. This metadata is the equivalent of a black box recording in aviation; and hospitals cannot erase it.
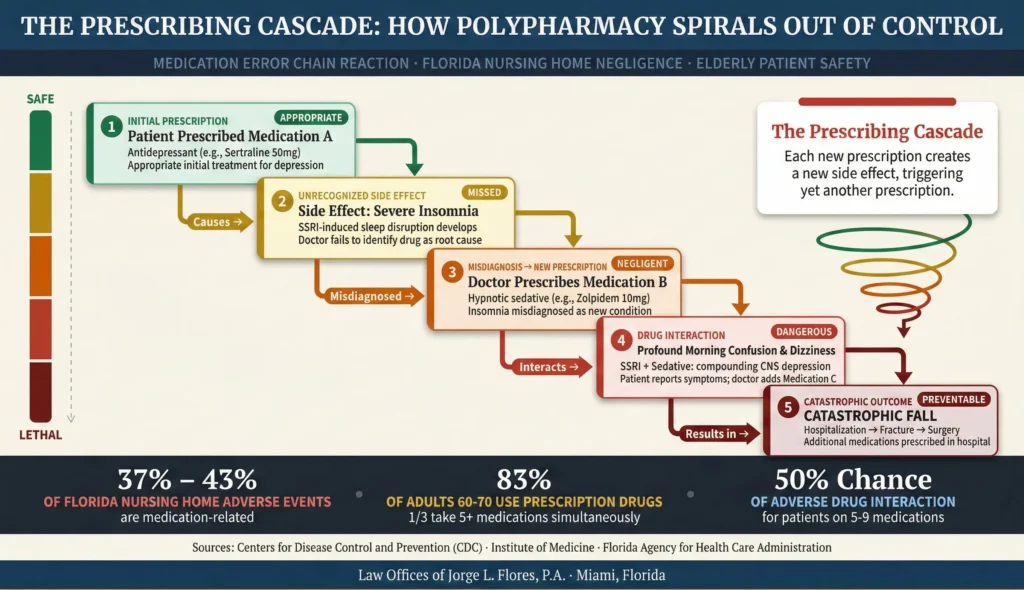
Polypharmacy; the simultaneous use of multiple prescription medications by a single individual; is particularly relevant in Florida due to the state’s vast demographic of elderly residents. According to the CDC, an astonishing 83% of adults in their 60s and 70s have used at least one prescription drug in the past 30 days, and approximately one third regularly take five or more simultaneously. Clinical studies indicate that patients taking five to nine distinct medications face a massive 50% chance of experiencing an adverse drug interaction. Inappropriate polypharmacy frequently triggers what is known as a “prescribing cascade”; an initial medication causes an adverse side effect, the physician misdiagnoses the side effect as a new condition and prescribes a second medication, and the drugs interact to cause catastrophic harm. In Florida nursing homes, medication errors account for an estimated 37% to 43% of all adverse events that result in harm to residents.
If you suspect a medication error caused your injury, contact the Law Offices of Jorge L. Flores, P.A. for a confidential consultation before critical evidence is lost.
FLORIDA LEGAL FRAMEWORK
The independent duty of the Florida pharmacist has evolved dramatically over the past two decades. Under the antiquated 1965 precedent of McLeod v. W.S. Merrell Co., a Florida pharmacist’s legal duty was incredibly narrow; merely to use due care in compounding the drug. That legal landscape has been fundamentally altered. In the paradigm shifting decision of Powers v. Thobani (2005), the Fourth District Court of Appeals determined that pharmacists have a legal duty to evaluate the “operative risks” of medications and to aggressively intervene when asked to fill repeated, unreasonable prescriptions with potentially fatal consequences. This was cemented by Oleckna v. Daytona Discount Pharmacy (2015), where the appellate court explicitly rejected “robotic compliance” with a physician’s instructions. Today, a Florida pharmacist who fills a fundamentally unreasonable prescription without questioning the prescriber is independently liable for pharmacy malpractice.
What This Means for Pharmacy Error Victims
If your pharmacy filled a prescription that was clearly dangerous on its face; a contraindicated drug combination, an extreme pediatric dosage, overlapping refill frequencies that should have raised red flags; the pharmacist is not protected by the argument that they were “just following the doctor’s orders.” Under Florida law, the pharmacist carries an independent legal duty to question the prescriber, counsel the patient, or refuse to fill the script. That means you can sue the pharmacy separately from the doctor.
Florida’s comparative fault framework under Section 768.81(3) of the Florida Statutes requires the court to enter judgment against each liable party solely on the basis of that specific party’s percentage of fault. Florida bans “joint and several liability” in negligence actions. However, Section 768.81(6) provides a critical exception: the 2023 legislative rule barring plaintiffs from recovering if found more than 50% at fault does not apply to medical negligence actions brought under Chapter 766. Medical malpractice victims may still recover their proportionate share of damages even if assigned the majority of the blame. For the full pre suit requirements, the types of damages available, and the 2025 caps ($750,000 per claimant, $1.5 million for catastrophic injuries, economic damages uncapped), see the linked guides.
Inside Advantage
Attorney Flores worked as an attorney for a top rated insurance defense firm in Miami, where he learned first hand how hospitals and their insurers defend medication error claims. He knows how defense teams weaponize “alert fatigue” arguments to deflect blame from individual physicians onto hospital IT systems. He knows how they aggressively use comparative fault to shift liability onto the patient. And he knows how they bury the override data deep in the EHR metadata where they believe plaintiffs’ attorneys will never look. That experience is why every medication error case we build starts with subpoenaing the raw electronic data and reconstructing every link in the chain of custody until we identify precisely where the system failed.
“As a former insurance defense attorney, I know exactly how hospitals and pharmacies defend these cases. They will bury the override data, blame the patient’s underlying condition, and characterize a preventable catastrophe as an ‘unavoidable side effect.’ We do not allow that to happen. We subpoena the EHR metadata, retain board certified pharmacologists, and reconstruct every link in the chain of custody until we identify precisely where the system failed.”
Jorge L. Flores, Esq.
You trusted the system. The system failed you. If you or a loved one has suffered catastrophic harm as a result of a wrong medication, a dosing error, a pharmacy dispensing mistake, or a failure to monitor drug toxicity, the experienced Law Offices of Jorge L. Flores, P.A., can help.
From our offices in Miami, Florida, we subpoena the EHR metadata, retain board certified pharmacologists and toxicologists, and reconstruct every link in the chain of custody. We handle medication error cases on a contingency basis; you pay nothing unless we recover for you.
P.S. Patients who have suffered a medication error oftentimes blame themselves; wondering if they should have asked more questions, read the label more carefully, or somehow caught the mistake before it was too late. Stop blaming yourself. The entire chain of custody exists precisely because the responsibility for medication safety rests on the healthcare professionals; not on you. The Law Offices of Jorge L. Flores, P.A., is here to hold them accountable.
Related: Medical Malpractice · Nursing Malpractice · Who Can Be Held Responsible · Types of Compensation · Pre Suit Requirements