

Reviewed by Jorge L. Flores, Esq. · Law Offices of Jorge L. Flores, P.A. · Miami, Florida · Last Updated: March 2026
Your medical record is the single most important piece of evidence in a malpractice case. It is also the piece of evidence you have the legal right to obtain yourself, right now, without an attorney, without a court order, and without paying more than $6.50 for an electronic copy.
The medical chart transforms from a clinical tracking tool into primary legal evidence the moment an adverse event occurs. Hospitals know this. Their risk management teams know this. And the speed at which you secure a complete, unaltered copy of that record can determine whether critical data is preserved or quietly overwritten. The Law Offices of Jorge L. Flores, P.A., in Miami, Florida, issues a records preservation letter on every case we investigate.
REQUEST YOUR RECORDS TODAY; DO NOT WAIT
Submit a written request for your complete electronic health record to every facility involved in your care; not just “the hospital.” Send separate requests to the ER physician group, the anesthesia group, the radiology provider, and the pathology lab. Specify that you want the EHR audit trail, the nursing flowsheets, the medication administration records, and the native DICOM imaging. Under HIPAA, providers must respond within 30 days. The electronic copy costs $6.50 or less. Do not accept a $500 paper invoice; demand the electronic version. Contact an attorney immediately so we can issue a formal preservation demand before routine IT purges destroy the audit trail data.
YOUR RIGHTS UNDER FLORIDA AND FEDERAL LAW
You have the legal right to a copy of your complete medical record.
Under HIPAA (45 CFR Section 164.524) and Florida Statute Section 456.057, healthcare providers must furnish a copy upon written request. The provider owns the physical record; you own the right to the information inside it.
Providers must respond within 30 days.
One 30 day extension is permitted if the provider notifies you in writing within the initial window. Florida law prohibits hospitals from delaying production for internal “legal review.”
A doctor cannot withhold your records because you owe money.
Section 456.057 explicitly prohibits conditioning the release of records on payment of outstanding clinical bills.
You are entitled to the actual images, not just the radiologist’s report.
Request imaging in DICOM format on a CD or via secure digital transfer. The written report is the radiologist’s opinion; the original image is the evidence.
Amendment 7 gives you the constitutional right to adverse incident reports.
Florida Constitution Article X, Section 25 grants patients access to records relating to any “adverse medical incident,” including peer review materials and internal risk management reports that were historically shielded. For a detailed explanation of how this applies in hospital negligence cases, see our dedicated guide.
WHAT IT ACTUALLY COSTS
| Source | Paper Records | Electronic Records |
|---|---|---|
| Hospital (Section 395.3025) | $1.00/page. Search fee: $1.00/year requested. | Request electronically under HIPAA: flat $6.50 or actual labor cost. |
| Physician Office (64B8-10.003) | $1.00/page first 25 pages; $0.25/page after. | $6.50 flat under HIPAA if maintained in EHR. |
| Imaging (DICOM) | N/A | Hospital: $20 handling + reproduction cost. Physician: $10 handling. |
| Continuity of Care | $0. Free. If the records are being copied for the purpose of continuing your medical care, Florida law prohibits charging any fee. | |
The $6.50 Rule Most Patients Do Not Know About
If a hospital sends you a $500 invoice for a 500 page paper chart, demand the records electronically instead. Under the 2016 HHS guidance on HIPAA access, if the records are maintained in an EHR system (and nearly all are), the provider may charge a flat fee of $6.50 for an electronic copy.
WHO YOU MUST REQUEST RECORDS FROM
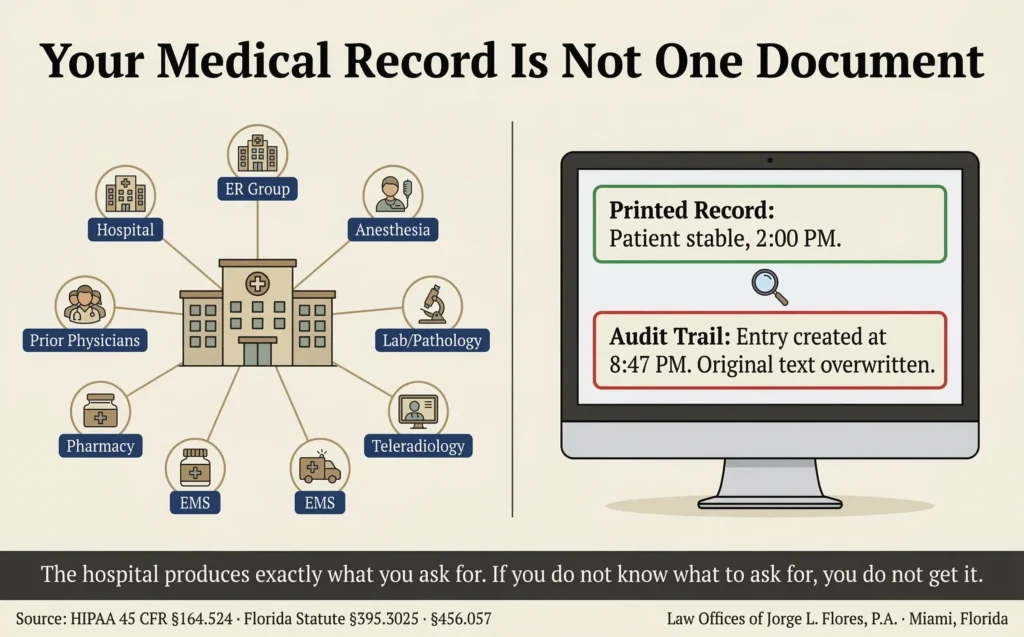
Requesting records from “the hospital” does not give you the complete picture. Modern healthcare is fractured across independent contractor groups that maintain separate records.
| Entity | What They Hold That the Hospital Does Not |
|---|---|
| The Hospital Facility | Inpatient nursing notes, ER triage records, hospital owned outpatient procedure documentation. |
| ER Physician Group | ER doctors are rarely hospital employees. Their independent group maintains separate clinical records and billing. |
| Anesthesia Group | Pre anesthesia evaluations, intraoperative management logs, PACU recovery notes. Oftentimes in a proprietary system separate from the hospital’s EHR. |
| Pathology / Outside Lab | Complete tissue biopsy workups and culture results. The hospital may only have a summarized result. |
| Teleradiology Provider | After hours and subspecialty imaging interpretations, communication logs, and image archives. Frequently a national company the patient never knew existed. |
| EMS / Ambulance | The earliest vital signs, cardiac rhythms, and neurological assessments. Establishes baseline before hospital admission. |
| Pharmacy | Independent dispensing logs that verify what medications were actually prescribed and received. |
| Prior Treating Physicians | Historical records establishing baseline health. The defense will use pre existing conditions against you. |
Why This List Matters
The anesthesiologist who managed your airway, the radiologist who read your scan, and the ER physician who triaged you oftentimes work for completely separate companies. Their records exist in separate systems. If you only request from “the hospital,” you will receive a chart with critical gaps that the defense will exploit.
If you suspect your records have been altered, contact the Law Offices of Jorge L. Flores, P.A. immediately.
PROTECTING THE EVIDENCE: AUDIT TRAILS AND PRESERVATION
The printed medical record shows you what the final version of the chart says. The EHR audit trail shows you when it was actually written, who wrote it, and what it said before it was changed.
|
What the Printed Record Shows A polished, chronological narrative. “Patient resting comfortably, no acute distress” charted at 2:00 PM. Vital signs normal. No documentation of deterioration. |
What the Audit Trail Reveals The “2:00 PM” entry was actually typed at 8:47 PM; six hours after the patient had already suffered a cardiac arrest and was transferred to the ICU. The original entry, overwritten at 8:47 PM, documented “patient unresponsive, code called.” |
The Records Preservation Letter
A preservation letter puts the hospital on formal notice that a potential claim exists and creates an immediate legal duty to halt all automated deletion protocols and preserve every record, audit trail, native DICOM image, and piece of physical equipment related to your care. If evidence disappears after the hospital receives a preservation letter, the court can instruct the jury to presume the destroyed evidence proved negligence.
Inside Advantage
Most law firms request “the medical record” and receive an abstract; a curated summary containing discharge notes, operative reports, and major consultations. Before founding this firm, Attorney Flores reviewed incoming records requests from the defense side and knows exactly what hospitals omit when they send the standard package. We do not request “the medical record.” We request every individual component by name; including the audit trail, the native DICOM images, the pharmacy dispensing logs, and the communication records between nursing and the on call physician. The hospital produces exactly what you ask for. If you do not know what to ask for, you do not get it.
The One Thing to Remember
The hospital produces exactly what you ask for. Not more. If you request “the medical record,” you will receive an abstract that omits the granular data where negligence hides. If you request the nursing flowsheets, the medication administration records, the EHR audit trail, and the native DICOM imaging by name, you will receive the evidence that actually proves the case.
If you need help securing your complete medical record, preserving audit trail evidence, or investigating whether records have been altered, the experienced Law Offices of Jorge L. Flores, P.A., can help.
We issue the preservation letter, request every component by name, subpoena the EHR audit trails, and retain forensic experts to identify alterations. All costs are advanced. You pay nothing unless we recover.
P.S. If you are reading this page because something went wrong during your medical care, request the complete electronic health record today. Do not wait for an attorney. Do not wait for the hospital to contact you. Florida law entitles you to a copy, and the longer you wait, the greater the risk that routine IT purges destroy the audit trail data that could prove your case. Call the Law Offices of Jorge L. Flores, P.A., after you have the records in hand; because the evidence is safest when it exists in more than one place.
Related: Medical Malpractice · Pre Suit Requirements · Complication vs. Negligence · Nursing Malpractice · Hospital Negligence