

Former hospital defense attorney · Law Offices of Jorge L. Flores, P.A. · Miami, Florida
Last Updated: April 2026
Acute Compartment Syndrome Is a Surgical Emergency. Every Hour of Delay Destroys Muscle and Nerve That Cannot Be Regrown.
Acute compartment syndrome develops when pressure inside a closed fascial compartment of the body, most commonly in the leg or forearm, rises to a level that cuts off blood flow to the muscles and nerves inside. It is one of the few true orthopedic and surgical emergencies. The only effective treatment is fasciotomy: a surgical incision that releases the pressure. Published orthopedic literature establishes that fasciotomy within six hours of the onset of ischemia is associated with full functional recovery, while delays beyond eight hours produce muscle necrosis, and delays beyond 12 hours produce permanent contractures, nerve damage, and in the most severe cases, amputation.
The diagnosis is not subtle. Every medical student is taught the classical presentation, known as the “five Ps”: pain out of proportion to the injury, paresthesia (numbness or tingling), pallor, pulselessness, and paralysis.
In reality, the first P, pain out of proportion, is the earliest and most reliable warning, and it is often the one the ER or orthopedic team dismisses as “normal post-operative pain” or the expected result of a fracture. By the time the other Ps appear, the window for full recovery has often closed.
In the compartment syndrome cases we handle in Miami, the pattern is consistent. The patient reported escalating pain that did not respond to narcotic medication. The nursing notes documented the complaints. The compartment pressure measurements, when they were finally taken, confirmed the diagnosis. But by that point, hours had passed, and the muscle inside the compartment was already dying. The records show exactly when the pain was first reported, when the team finally responded, and how long the gap was.
⚠ The Fasciotomy Window Closes Fast. The Legal Window Has Deadlines Too.
Florida’s statute of limitations for medical malpractice is generally two years from the date of discovery, with a four year statute of repose in many cases, though specific deadlines can vary based on the facts and statutes in effect. For wrongful death, the limitations period generally runs two years from the date of death. The nursing flowsheets, pain score entries, compartment pressure measurements, and order logs can be overwritten if not preserved early.
Free Case Review: Was the Fasciotomy Delayed? (305) 598-2221
Compartment Syndrome May Have Been Missed If:
✓ You or your family member repeatedly reported severe pain “out of proportion” to the injury or surgery and were told it was normal and given more pain medication.
✓ The affected limb became tight, swollen, numb, pale, or cold before anyone measured the compartment pressure or called for an orthopedic or vascular consult.
✓ A cast, splint, or surgical dressing was not loosened despite escalating pain and swelling underneath it.
✓ Compartment pressure was eventually measured and showed elevated values, but hours had already passed since the first complaints were documented.
✓ Fasciotomy was finally performed, but the muscle was already dead and permanent nerve damage, contractures, or amputation followed.
If any of these describe what happened at a Miami hospital, the nursing pain scores, the compartment pressure measurements, and the order timestamps deserve an independent review. We arrange that review at no cost.
On This Page
How Compartment Syndrome Develops and the High-Risk Scenarios
The Five Ps and the Pressure Measurement That Confirms the Diagnosis
The Fasciotomy Clock: Three Windows Where the Delay Produced Permanent Damage
Who Is Liable When Compartment Syndrome Is Missed
Volkmann’s Contracture, Amputation, and the Lifetime Cost of a Preventable Injury
HOW COMPARTMENT SYNDROME DEVELOPS AND THE HIGH-RISK SCENARIOS
Compartment syndrome is not a surprise diagnosis. It develops in clinical contexts that are well recognized in orthopedic, trauma, and emergency medicine training. When a patient presents with any of the following, the treating team is on notice that compartment syndrome is a foreseeable complication and must be actively monitored for.
Tibial shaft and forearm fractures. These are the single most common triggers. The tibial shaft fracture alone accounts for a substantial share of acute compartment syndrome cases in adults, and high-energy fractures, crush injuries, and fractures with significant displacement carry the highest risk. When a Miami ER or orthopedic team admits a patient with a tibial shaft fracture, compartment syndrome monitoring is part of the expected standard of care, not an optional step.
Crush injuries, high-energy trauma, and reperfusion after prolonged ischemia. A limb crushed under a heavy object, trapped after a vehicle accident, or reperfused after vascular repair is at particularly high risk because tissue swelling can develop rapidly once circulation is restored. The trauma documentation, the prehospital records, and the OR time for vascular repair all provide the clinical context that should have triggered heightened surveillance.
Casts, splints, and tight circumferential dressings. A well-intentioned immobilization device can itself create the pressure problem. If the patient complains of escalating pain or numbness beneath a cast and the cast is not bivalved, split, or removed to evaluate the underlying tissue, the cast becomes a contributing factor. The nursing notes and the provider notes document whether the complaint was recognized and whether the dressing was modified in response.
Orthopedic and vascular surgery, including intramedullary nailing and arterial repair. Post-operative compartment syndrome is a recognized complication. Patients are supposed to be monitored with serial neurovascular checks in the post-operative period. When those checks are documented as “within normal limits” every hour despite escalating patient complaints, either the documentation is not accurate or the person performing the check was not looking for what should have been found.
THE FIVE PS AND THE PRESSURE MEASUREMENT THAT CONFIRMS THE DIAGNOSIS
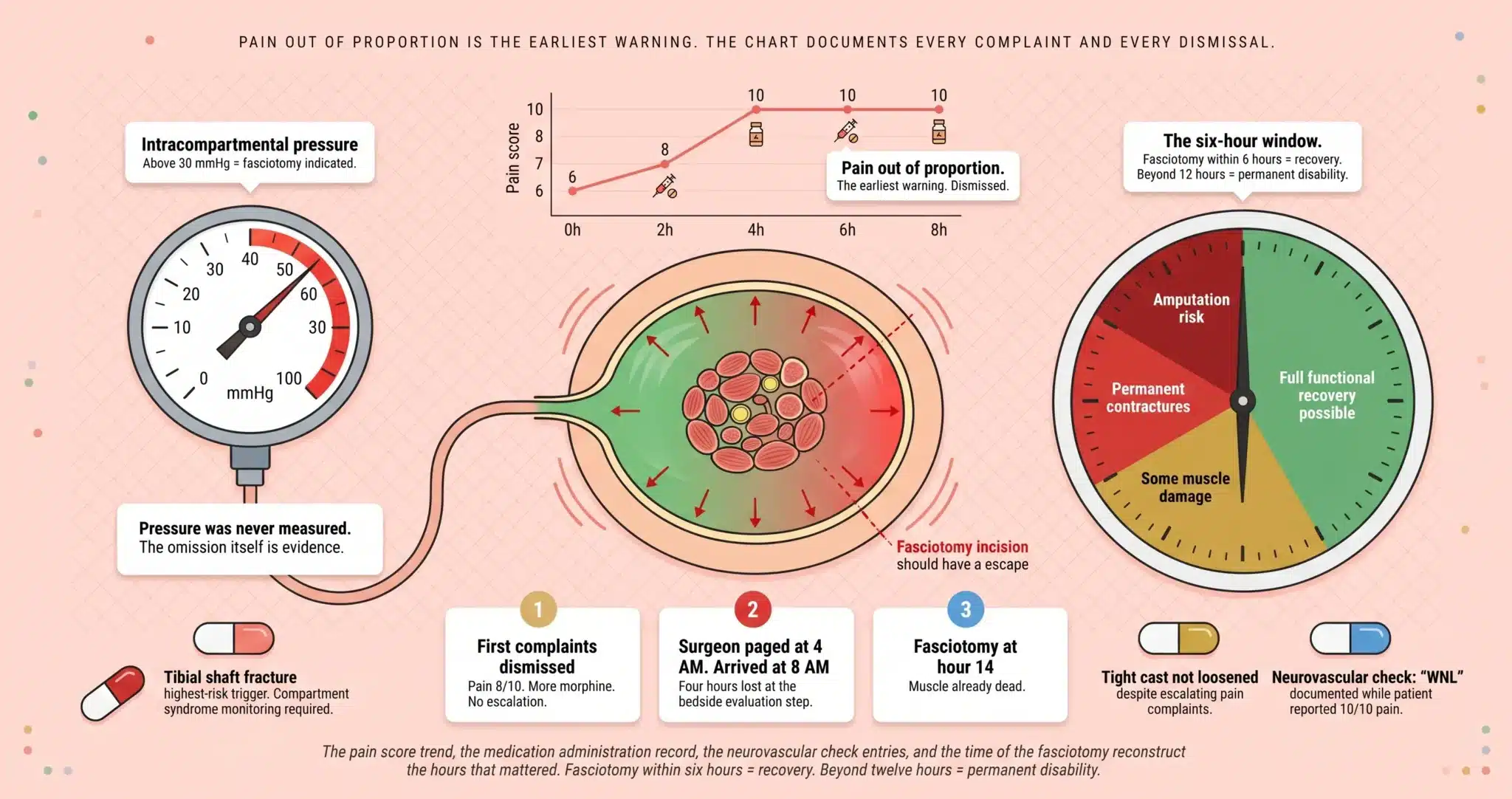
Pain out of proportion to the injury is the earliest clinical sign and the most important one. It means the patient’s reported pain level is greater than what would be expected for the underlying fracture, surgery, or injury, and it does not respond adequately to standard doses of opioid pain medication. Pain scores in the EMR are recorded at regular intervals. When pain scores climb from 6 to 8 to 10 over a few hours despite escalating medication, the pattern is visible in the chart before any other symptom appears.
Pain with passive stretch of the muscles in the affected compartment is the most specific physical examination finding. Dorsiflexion of the foot in anterior leg compartment syndrome, extension of the fingers in forearm compartment syndrome, these maneuvers should reproduce severe pain. A nurse or physician performing a neurovascular check who does not test passive stretch, or who tests it and does not document the result, has failed to perform the exam the situation required.
Paresthesia, pallor, paralysis, and pulselessness are later findings. By the time these appear, the nerves and muscles inside the compartment have been ischemic for hours. Pulselessness is often misunderstood as an early sign. It is not. A palpable pulse can be present even in an established compartment syndrome because the arterial pressure inside the major vessel may remain higher than the compartment pressure until late in the course. Waiting for pulselessness means waiting too long.
Compartment pressure measurement is the objective test. When clinical suspicion exists, particularly in patients who cannot reliably report pain (sedated, intubated, under regional anesthesia, or with nerve blocks that mask symptoms), intracompartmental pressure can be measured directly with a handheld device. An absolute pressure above 30 mmHg, or a delta-pressure (diastolic blood pressure minus compartment pressure) less than 30 mmHg, is the published threshold that supports the diagnosis and the decision to proceed to fasciotomy. When compartment pressure was never measured in a high-risk patient with escalating pain, the omission is itself evidence of a diagnostic failure.
THE FASCIOTOMY CLOCK: THREE WINDOWS WHERE THE DELAY PRODUCED PERMANENT DAMAGE
Window 1: The First Complaints That Were Dismissed
The pain score was 6 when the patient returned from the OR. Two hours later it was 8. Four hours later it was 10. The patient told the nurse the pain was not improving despite morphine. The patient’s family told the nurse something was wrong.
The nurse gave another dose, documented “patient resting in bed,” and did not call the surgeon. Our orthopedic and emergency medicine experts identify the first documented entry that should have triggered escalation and mark the minute at which the diagnosis should have been suspected, not the minute at which it was actually made.
Window 2: The Delay Between Suspicion and Pressure Measurement
Once the clinical picture raises compartment syndrome as a diagnostic possibility, the next step is either direct measurement of compartment pressure or expedited surgical consultation. The order timestamp for the compartment pressure measurement, the time the measurement was performed, and the value recorded are all in the chart. If the surgeon was paged at 4 AM and did not come to the bedside until 8 AM, the four hours between the page and the evaluation are in the call log. Every segment of this interval is attributable to a specific individual and, in some cases, to the institution’s on-call coverage structure.
Window 3: The Interval From Diagnosis to Fasciotomy
Once compartment syndrome is confirmed, the fasciotomy must be performed emergently. The decision to take the patient to the OR, the time the OR was booked, the anesthesia record, and the incision time are all documented. In the compartment syndrome cases we handle across Miami-Dade County, the most damaging delay is often the gap between the diagnostic decision and the skin incision, measured in hours rather than the minutes the literature supports. Every hour the tissue spent ischemic is measurable against the orthopedic literature on functional recovery.
WHO IS LIABLE WHEN COMPARTMENT SYNDROME IS MISSED
The orthopedic surgeon responsible for the patient’s fracture care has a direct duty to monitor for compartment syndrome and to respond when warning signs are documented. The emergency department physician who initially evaluated the patient has the same duty during the ED workup of a high-risk injury.
Bedside nurses and charge nurses are responsible for neurovascular checks, accurate documentation of pain scores, and escalation to the physician when the clinical picture changes. A nurse who documents “pain controlled” while the patient and family are reporting the opposite has created a record that conflicts with the reality, and that conflict becomes part of the case.
The hospital as an institution may be liable for on-call coverage arrangements that produce predictable delays, for post-operative monitoring protocols that do not include compartment syndrome surveillance for high-risk patients, and for staffing decisions that leave one nurse responsible for too many post-surgical patients to perform the hourly neurovascular checks the standard of care requires.
VOLKMANN’S CONTRACTURE, AMPUTATION, AND THE LIFETIME COST OF A PREVENTABLE INJURY
The consequences of missed or delayed fasciotomy span a spectrum. Mild cases may produce chronic pain, weakness, and reduced function in the affected limb. Moderate cases produce Volkmann’s ischemic contracture: permanent shortening and deformity of the muscles and tendons that leaves the hand or foot in a fixed, non-functional position. Severe cases produce extensive muscle necrosis requiring debridement, nerve damage that does not recover, and in the worst outcomes, amputation.
In the most catastrophic cases, massive muscle breakdown produces rhabdomyolysis and acute kidney failure, sometimes requiring dialysis, and the systemic inflammatory response can progress to multi-organ failure and death. For a young, previously healthy patient, the difference between a fasciotomy performed in six hours and one performed in 14 hours can be the difference between a full return to work and lifelong disability.
The Life Care Plan in a compartment syndrome case projects the cost of reconstructive surgery, tendon transfers, prosthetics if amputation resulted, physical and occupational therapy for years, pain management, psychological support for the trauma of a preventable disability, home and vehicle modifications, and attendant care at the level the residual deficits require. A forensic economist calculates lost income and diminished earning capacity over the patient’s remaining working life. The total is built from documented necessity, not speculation.
How the Defense Uses Opioid Tolerance and Subjective Pain to Shift the Blame to the Patient
The defense tactic in compartment syndrome cases is to attack the patient. Their expert will testify that the patient had a “low pain tolerance,” a history of opioid use that made their pain reports unreliable, or a history of drug-seeking behavior that the nursing team reasonably considered when deciding not to escalate. They will argue the patient’s pain was subjective and the team’s response was proportionate to objective findings that were not yet present. Attorney Jorge L. Flores saw this strategy constructed during the years he spent at a Miami insurance defense firm, where defense teams built patient-blame narratives from the moment the chart first mentioned a high pain score.
This defense collapses on contact with the literature. Pain out of proportion is not a subjective complaint. It is a recognized diagnostic criterion that orthopedic and emergency medicine textbooks teach as the earliest warning sign of compartment syndrome. The published standard does not say “believe the patient only if their pain tolerance appears normal.” It says high-risk patients with escalating pain require neurovascular examination, passive stretch testing, and compartment pressure measurement when clinical suspicion is present.
Jorge Flores builds every compartment syndrome case to eliminate the “unreliable patient” exit. He presents the pain score trend, the medication administration record showing escalating doses without corresponding pain reduction, and the orthopedic literature establishing that exactly this pattern is the diagnosis until proven otherwise. The patient is not the defendant. The team that failed to perform the exam the pattern demanded is.
Pain Out of Proportion Is the Earliest Warning. The Chart Documents Every Complaint and Every Dismissal.
The pain score trend, the medication administration record, the neurovascular check entries, and the time of the fasciotomy reconstruct the hours that mattered. If the window was missed, the evidence is already in the record.
(305) 598-2221
FREQUENTLY ASKED QUESTIONS
What is acute compartment syndrome and why is it an emergency?+
Acute compartment syndrome is a rapid rise in pressure inside a closed fascial compartment, usually in the leg or forearm, that cuts off blood supply to the muscles and nerves within it. Untreated, the tissue dies within hours. The only effective treatment is a fasciotomy, a surgical incision that releases the pressure. Because the muscle and nerve damage is irreversible once it occurs, the diagnosis must be made and surgery must be performed within a narrow window for the patient to recover full function.
Is every missed diagnosis of compartment syndrome malpractice?+
No. Compartment syndrome can develop subtly in patients who are sedated, under regional anesthesia, or otherwise unable to report pain, and even competent teams may face genuinely difficult diagnostic situations. A missed diagnosis becomes malpractice when the clinical picture gave the team the information they needed to suspect the diagnosis and measure compartment pressure, and they failed to do so within the timeframe the published standard of care required. The difference between a difficult case and a negligent one is documented in the pain scores, the neurovascular checks, and the response to escalating complaints.
How much time does the surgical team have before the damage becomes permanent?+
Published orthopedic literature consistently establishes that fasciotomy performed within six hours of ischemia onset is associated with the best functional outcomes. Between six and eight hours, some muscle damage may occur but is often recoverable. Beyond eight to 12 hours, significant muscle necrosis and nerve damage are likely. Beyond 12 hours, permanent contractures, chronic pain, and potentially amputation become increasingly probable. The specific numbers depend on the compartment involved and the severity of the ischemia.
What if the nurse or doctor said my pain was “just anxiety” or I was “drug seeking”?+
These characterizations are common in compartment syndrome cases where the diagnosis was missed, and they are also the first line of defense in litigation. The orthopedic and emergency medicine literature is clear that high-risk patients with pain out of proportion require objective evaluation (neurovascular exam, passive stretch testing, and compartment pressure measurement when indicated), not clinical judgment based on a guess about the patient’s psychology or drug history. The chart documents whether the objective evaluation was performed.
How long do I have to file a compartment syndrome case in Miami?+
Florida’s statute of limitations for medical malpractice is generally two years from the date you knew or should have known the injury was caused by substandard care, with a four year statute of repose in many cases, though specific deadlines can vary based on the facts and statutes in effect. For wrongful death, the limitations period generally runs two years from the date of death. The nursing flowsheets, pain score entries, and compartment pressure measurements are stored on the hospital’s systems and can be overwritten. Contacting us early allows us to issue preservation demands before the evidence is lost.
What does it cost to hire a lawyer for a compartment syndrome case?+
The firm carries every cost of the case from the first record request through trial. The medical record retrieval, the orthopedic and emergency medicine expert reviews, the Life Care Plan, and the forensic economics report are all funded by us. We collect a fee only when compensation is recovered. If the case does not produce a result, the investment was entirely ours.
CONTACT US FOR A FREE CASE REVIEW
If you or a family member suffered permanent disability or amputation from a compartment syndrome that a Miami hospital failed to diagnose in time, the Law Offices of Jorge L. Flores, P.A., will review the pain score trend, the nursing neurovascular checks, the compartment pressure measurements, and the operative timeline at no charge. We tell families what the evidence shows. That conversation costs nothing and commits you to nothing.
Free Case Review. No Cost Unless We Recover Compensation.
We fund the records, the expert consultations, and the full investigation. Our fee is contingent on the outcome.
(305) 598-2221
Or submit your information below and we will contact you within 24 hours.
Your information is confidential. Submitting this form does not create an attorney-client relationship.
Prefer to speak directly? Call (305) 598-2221 for an immediate consultation.
Related: Medical Malpractice · Post-Operative Complications · Unnecessary Surgery · Wrongful Death