

Former hospital defense attorney · Law Offices of Jorge L. Flores, P.A. · Miami, Florida
Last Updated: April 2026
The Surgery May Have Gone as Planned. What Happened Afterward Is Where the Negligence Lives.
Complications after surgery are not always malpractice. Bleeding, infection, and clots are known risks that patients are warned about before they sign the consent form. But when those complications produce warning signs that appear in the vital signs, the lab results, and the nursing notes, and the medical team does not respond until the patient is in crisis, the harm is no longer a complication of the surgery. It is a consequence of the delay. The distinction matters because the case is not about whether the surgery should have been performed. It is about what the team did with the information the monitors and the chart were giving them in the hours and days that followed.
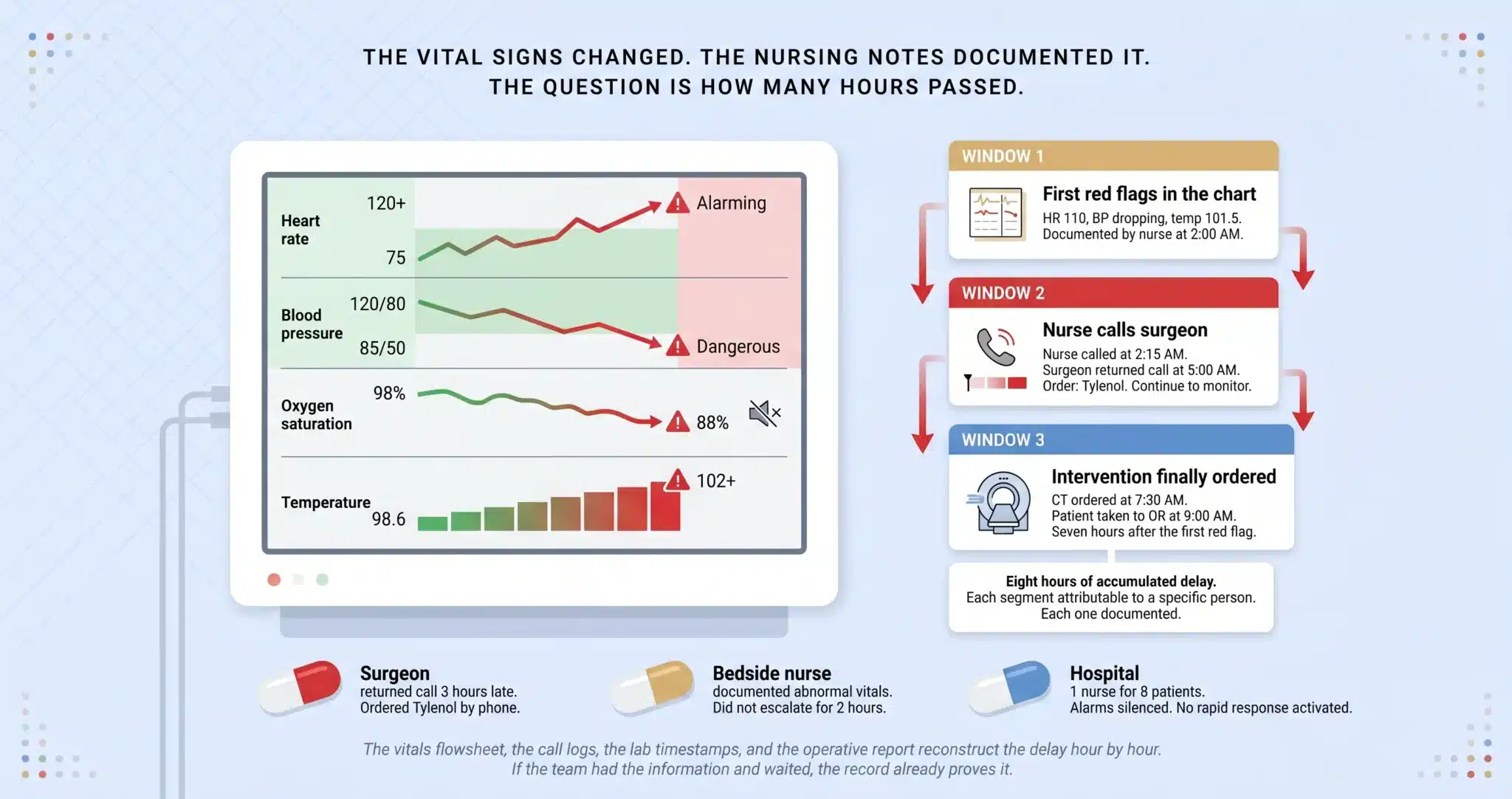
In the post-operative negligence cases we handle across Miami, the pattern is consistent. The vital signs change first. Heart rate climbs. Blood pressure drops. Temperature spikes. Oxygen saturation drifts downward. The nursing notes document these changes in real time. The question is how long those changes persisted before someone picked up the phone and called the surgeon, how long it took the surgeon to evaluate the patient after that call, and how long it took to order the CT, the labs, or the return to the operating room that the clinical picture demanded. Every one of those intervals is timestamped in the electronic medical record.
⚠ The Vital Signs Changed Before the Patient Crashed. The Chart Proves When.
Florida’s statute of limitations for medical malpractice is generally two years from the date of discovery, with a four year statute of repose in many cases, though specific deadlines can vary based on the facts and statutes in effect. For wrongful death, the limitations period generally runs two years from the date of death. Hospital EMR data, vitals flowsheets, and nursing call logs can be overwritten if not preserved early.
The Post-Operative Response May Have Failed If:
✓ You or your family repeatedly reported worsening pain, swelling, shortness of breath, or confusion after surgery and were told “that is normal recovery.”
✓ Vital signs including heart rate, blood pressure, temperature, oxygen level, or urine output were abnormal for hours before anyone escalated care.
✓ Lab results showed a rising white blood cell count, elevated lactate, dropping hemoglobin, or worsening kidney function but no additional tests, antibiotics, or imaging were ordered.
✓ A treatable complication such as internal bleeding, surgical site infection, bowel leak, blood clot, or compartment syndrome was finally identified, but only after days of visible decline.
✓ Your family member was discharged home and returned to the ER within days with sepsis, organ failure, or a condition that was developing before discharge.
If any of these describe what happened after surgery at a Miami hospital, the post-operative records deserve an independent review. We arrange that review at no cost.
On This Page
The Post-Operative Complications We See Mishandled Most Often
The Deterioration Timeline: Three Windows Where the Response Broke Down
Handoff Failures, Ignored Alarms, and AI Monitoring That Was Not Used
How We Reconstruct the Post-Operative Timeline From the Hospital’s Own Records
Who Is Liable When the Post-Operative Team Fails to Respond
THE POST-OPERATIVE COMPLICATIONS WE SEE MISHANDLED MOST OFTEN
Internal bleeding and hemorrhage. Blood pressure drops. Heart rate rises. Hemoglobin falls on serial labs. The surgical drain output changes color or volume. The abdomen becomes distended and firm. Each of these findings is documented in the post-operative flowsheet. When they appear together and the team does not order a stat hemoglobin, a CT with contrast, or an emergent return to the operating room, the delay between the first abnormal vital sign and the intervention is the core of the case.
Surgical site infection and sepsis. Fever that persists beyond the first 48 hours. White blood cell count climbing on serial labs. Heart rate above 100. Lactate rising. Mental status changing from alert to confused. These are the systemic inflammatory response criteria that should trigger blood cultures, broad-spectrum antibiotics, imaging to locate the source, and in many cases surgical drainage or washout. When the post-operative team attributes a fever to “expected post-surgical inflammation” for three days and the patient develops septic shock, the nursing notes and the vital sign trends document every hour the team had the information and did not act.
Anastomotic leak and bowel perforation. After abdominal surgery, a leak at the surgical connection point spills intestinal contents into the peritoneal cavity. The signs are escalating abdominal pain, fever, tachycardia, and free air on imaging. Delay in recognition turns a contained leak that could have been repaired into generalized peritonitis, sepsis, multi-organ failure, and death. The CT that would have confirmed the leak is often not ordered until the patient is already in the ICU.
Deep vein thrombosis and pulmonary embolism. Calf pain, swelling, and warmth after surgery. Sudden onset shortness of breath, tachycardia, chest pain, and dropping oxygen saturation. DVT prophylaxis with compression devices and anticoagulation is standard of care for surgical patients. When prophylaxis was not ordered, not administered, or was discontinued prematurely, and the patient throws a clot to the lungs, the medication administration record and the nursing documentation prove whether the protocol was followed.
THE DETERIORATION TIMELINE: THREE WINDOWS WHERE THE RESPONSE BROKE DOWN
No competitor in the current search results provides a structured deterioration timeline showing the gap between when a complication became apparent in the chart and when the clinical team finally acted. That gap is where post-operative negligence cases are built.
Window 1: The First Red Flags in the Chart
The vitals flowsheet is the foundation. Post-operative patients in Miami hospitals have vital signs recorded every one to four hours depending on acuity. The first abnormal reading, a heart rate that crosses 110, a systolic blood pressure that drops below 90, a temperature above 101.5, an oxygen saturation below 92, is timestamped. The nursing assessment notes that accompany the vital signs describe what the nurse observed: increased wound drainage, abdominal distention, mental status change, patient complaint of worsening pain. Our critical care experts identify the first documented deviation from the expected recovery trajectory and mark it as the point at which the standard of care required escalation.
Window 2: Nurse Escalation to the Surgeon or Hospitalist
When the nurse recognizes an abnormal trend, the standard of care requires notification of the responsible physician. The call log, the page system records, and the nursing notes document when the call was placed, what information was communicated, and what orders were received in response. If the nurse called at 2 AM and the surgeon returned the call at 5 AM, those three hours are documented.
If the surgeon gave a telephone order for Tylenol and told the nurse to “continue to monitor” without coming to the bedside to examine a patient whose hemoglobin had dropped two points in six hours, that telephone order is in the chart. If the nurse did not call at all despite documenting abnormal vitals, the absence of the call is its own evidence. Our nursing experts compare what was documented against what the standard of care required the nurse to communicate and when.
Window 3: The Decision to Order Tests, Transfer to ICU, or Return to Surgery
Once the surgeon evaluates the patient, the clock does not stop. If the clinical picture warrants a stat CT, the timestamp on the CT order, the time the study was performed, and the time the radiologist read it are all in the record. If the patient needed an emergent return to the operating room, the operative report documents when the case was booked, when anesthesia was called, and when the incision was made.
In the post-operative cases we handle in Miami-Dade County, the most damaging evidence is not one catastrophic delay. It is a cascade of incremental delays that compound: two hours before the nurse called, three hours before the surgeon arrived, another hour before the CT was ordered, another two hours before the patient was taken back to surgery. Eight hours of accumulated delay, each segment attributable to a specific individual or institutional failure, each one documented in a different section of the chart.
HANDOFF FAILURES, IGNORED ALARMS, AND AI MONITORING THAT WAS NOT USED
Shift change handoffs. The day nurse documented a rising heart rate and increasing wound drainage at 6 PM. The night nurse who took over at 7 PM did not receive that context, or received it and did not act on it. By midnight, the patient was in hemorrhagic shock. Handoff communication failures between nursing shifts, between the surgeon and the covering hospitalist, and between the floor team and the ICU are among the most frequent contributors to post-operative deaths. The handoff documentation, if it exists, shows what was communicated. If it does not exist, the absence is the evidence.
Monitor alarms that were silenced or ignored. Post-operative patients on continuous monitoring generate alarms for heart rate, oxygen saturation, blood pressure, and respiratory rate. Alarm fatigue, the phenomenon where clinical staff become desensitized to frequent alerts and silence them without evaluating the patient, is a recognized patient safety crisis. The monitor system logs every alarm, every acknowledgment, and every silence event. When a patient’s oxygen saturation alarmed at 88 percent 14 times over four hours and was silenced each time without a bedside evaluation, the alarm log is discoverable evidence of institutional failure.
Predictive deterioration tools and AI monitoring. Some Miami hospitals have implemented early warning score systems or AI-driven deterioration prediction platforms that analyze vital sign trends and flag patients at risk of clinical decline before the decline becomes obvious. If the hospital deployed such a system and it generated an alert that was not acted upon, or if the system was available but not activated for a post-surgical patient who should have been enrolled, the institutional negligence extends beyond the individual nurse or physician to the facility that purchased the technology and failed to use it.
HOW WE RECONSTRUCT THE POST-OPERATIVE TIMELINE FROM THE HOSPITAL’S OWN RECORDS
Every document listed below is generated automatically by the hospital’s own systems during the post-operative course. We demand them in their original electronic format, not the printed summary the hospital’s legal department selects. Lined up chronologically, they reconstruct the full deterioration timeline with minute-level precision.
Vitals flowsheets showing heart rate, blood pressure, temperature, oxygen saturation, respiratory rate, and urine output at every recorded interval. Nursing assessment notes describing wound appearance, pain level, mental status, drain output, and any patient or family concerns communicated to the nurse. Physician order logs with timestamps showing when labs, imaging, medications, and consults were ordered and by whom.
Lab result timestamps showing when blood was drawn, when results were available, and when the ordering physician acknowledged them in the system. Radiology order and read times showing the interval between the CT order, the study completion, and the radiologist’s final interpretation. Call and page logs documenting when the nurse contacted the surgeon or hospitalist and what response was received. Rapid response team activation records if one was called, or the absence of activation if one should have been. Monitor alarm logs and AI deterioration alert records if the hospital deployed predictive monitoring. We align these records on a single timeline and present it alongside our surgical and critical care experts’ opinion on when intervention should have occurred at each point.
WHO IS LIABLE WHEN THE POST-OPERATIVE TEAM FAILS TO RESPOND
The surgeon who performed the procedure has a post-operative duty to evaluate the patient when notified of concerning changes and to order appropriate tests or interventions without unreasonable delay. The hospitalist or intensivist covering the patient’s floor or ICU care carries the same obligation when the patient’s condition changes under their watch.
The bedside nurse and charge nurse are responsible for accurate monitoring, charting, and escalation. A nurse who documents abnormal vitals but does not notify the physician has created a record that proves the failure. A charge nurse who receives a bedside nurse’s concern and does not activate the chain of command shares the liability.
The hospital as an institution is responsible for staffing ratios, handoff protocols, alarm management policies, rapid response team availability, and the implementation and operationalization of monitoring technology. When a Miami hospital assigns a single nurse to eight post-surgical patients and a complication goes unrecognized because the nurse was physically unable to round on all eight within the required interval, the staffing decision is the institutional failure.
WHAT YOU CAN RECOVER WHEN THE DELAY MADE EVERYTHING WORSE
The damages in a delayed-response case are measured by the difference between what would have happened with timely intervention and what actually happened because the team waited. A post-operative bleed caught in two hours may require one return to the OR and a few extra days in the hospital. The same bleed caught in 12 hours may have produced hemorrhagic shock, organ damage, a prolonged ICU stay, and permanent disability.
Florida law permits recovery for the additional surgeries, the extended hospitalization, the ICU care, the rehabilitation, and the long-term medical needs that resulted from the delay rather than from the original procedure. Lost income during the extended recovery. Diminished earning capacity if the complications produced permanent impairment. Pain that would not have existed if the response had been timely. For wrongful death cases, the full measure of losses to the surviving family. A Life Care Planner and forensic economist project these costs with the same specificity we apply to every element of the case.
How the Defense Rewrites the Chart After the Fact and What We Do About It
In post-operative failure-to-respond cases, the defense does not just argue the response was reasonable. It argues the chart tells a different story than the family experienced. Attorney Jorge L. Flores knows this tactic because he watched hospitals execute it during the years he spent at a Miami insurance defense firm. Late addendums appear in the electronic medical record, backdated assessments are inserted, and nursing notes are amended to include language suggesting the team was “aware of” and “monitoring” the findings the family says were ignored.
Electronic medical record systems track every edit. Every addendum carries a timestamp showing when it was created, not when the event it describes occurred. A nursing note amended at 9 AM to describe an assessment that allegedly happened at 2 AM is visible in the EMR audit trail. Jorge Flores demands the full audit log in its native format, not the printout the hospital selects. He knows which fields are editable, which are locked, and which amendment patterns indicate contemporaneous documentation versus after-the-fact reconstruction. The chart can be rewritten. The audit trail cannot.
The Vital Signs Changed. The Nursing Notes Documented It. The Question Is How Many Hours Passed Before Anyone Acted.
The vitals flowsheet, the call logs, the lab timestamps, and the operative report reconstruct the delay hour by hour. If the team had the information and waited, the record already proves it.
(305) 598-2221
FREQUENTLY ASKED QUESTIONS
Is every complication after surgery considered malpractice?+
No. Bleeding, infection, and blood clots are recognized risks of surgery that patients are counseled about before the procedure. A complication becomes malpractice when the post-operative team had warning signs in the vital signs, labs, or physical examination, and failed to respond within a timeframe that a reasonably competent medical team would have met. The case is not about whether the complication occurred. It is about whether the team’s response to the complication met the standard of care.
What signs after surgery should nurses and doctors never ignore?+
Persistent tachycardia (heart rate above 100), hypotension (systolic blood pressure below 90), fever above 101.5 beyond 48 hours, dropping oxygen saturation, declining urine output, a hemoglobin that falls more than 2 points, rising lactate, altered mental status, increasing wound drainage or abdominal distention. Any combination of these findings in a post-surgical patient should trigger immediate physician notification, labs, and imaging. The vitals flowsheet documents whether they were present and when they were first recorded.
How do you prove it was the delay and not the original surgery that caused the harm?+
Our surgical and critical care experts compare the outcome that occurred with the outcome that would have been expected if the complication had been caught and treated within the window the clinical picture demanded. Published surgical literature provides benchmarks for response times and expected outcomes. If an anastomotic leak repaired within 12 hours of first symptoms has a mortality rate of 5 percent, and the same leak repaired at 72 hours has a mortality rate of 40 percent, the 60 hours of delay is the variable that changed the prognosis.
What if my family member was sent home and came back septic?+
Premature discharge after surgery is a recognized failure pattern. If the patient was sent home with vital signs or lab values that did not meet safe discharge criteria, or if the discharge occurred before post-operative milestones were achieved (return of bowel function after abdominal surgery, adequate pain control, stable hemoglobin), the discharge decision itself is part of the negligence claim. The discharge summary, the last set of vital signs, and the ER readmission records reconstruct whether the patient should have been sent home at all.
Can ignoring monitor alarms or AI deterioration alerts be malpractice?+
Yes. Monitor systems log every alarm and every acknowledgment. If a patient’s oxygen saturation alarmed repeatedly and was silenced without a bedside evaluation, the alarm log is evidence of a failure to assess. If the hospital deployed an AI-driven early warning system and the alert was generated but not acted upon, or the patient was not enrolled in the system when they should have been, the institutional negligence extends beyond the individual clinician to the facility’s operational failures.
How long do I have to file a post-operative malpractice case in Miami?+
Florida’s statute of limitations for medical malpractice is generally two years from the date you knew or should have known the post-operative care was negligent, with a four year statute of repose in many cases, though specific deadlines can vary based on the facts and statutes in effect. For wrongful death, the limitations period generally runs two years from the date of death. The post-operative vital signs, nursing notes, call logs, and alarm data are stored on the hospital’s systems and can be overwritten. Contacting us early allows us to issue preservation demands while the data is intact.
What does it cost to hire a lawyer for a post-operative negligence case?+
The firm bears every cost from the first record request through trial preparation. The EMR acquisition, the surgical and critical care expert consultations, the nursing standard-of-care review, the Life Care Plan, and the forensic economics analysis are all advanced by us. We collect a fee only if compensation is recovered for your family. If the case produces no result, the investment was ours entirely.
CONTACT US FOR A FREE CASE REVIEW
If your family member suffered a worsened outcome because a Miami hospital failed to respond to post-operative warning signs in time, the Law Offices of Jorge L. Flores, P.A., will review the surgical records, the vitals flowsheets, the nursing notes, and the call logs at no charge. We reconstruct the timeline and tell you whether the delays are supported by the evidence. That conversation costs nothing and obligates you to nothing.
Free Case Review. No Cost Unless We Recover Compensation.
We fund the records, the experts, and the full investigation. Our fee is contingent on recovering compensation for your family.
(305) 598-2221
Related: Medical Malpractice · Wrongful Death · Unnecessary Surgery · Aortic Dissection Misdiagnosis