

Former hospital defense attorney · Law Offices of Jorge L. Flores, P.A. · Miami, Florida
Last Updated: April 2026
A Prolapsed Cord Is an Emergency. A Delayed Response Is Malpractice.
The umbilical cord slips past the baby’s head and into the birth canal. Blood flow to the baby drops. The fetal heart rate plummets on the monitor. From this moment forward, every minute that passes without delivery is a minute of oxygen deprivation to the brain. The clinical team in a Miami delivery room has one job when a cord prolapse is identified: get the baby out. Not in an hour. Not after a conference with the attending. Now.
The medical literature is unambiguous. A cord prolapse requires emergency cesarean delivery. The interval between the prolapse event and the delivery of the baby is the variable that determines whether the child suffers a hypoxic brain injury or is born healthy. When that interval is extended by a team that hesitated, a hospital that did not have an anesthesiologist available, or a physician who attempted to manage the situation conservatively instead of moving to the operating room, the resulting brain damage was not caused by the prolapse. It was caused by the response to the prolapse.
⚠ Minutes Determined the Outcome. The Record Proves It.
If your child suffered a brain injury following an umbilical cord prolapse at a Miami hospital, the fetal monitoring strips and the operative report document exactly how many minutes elapsed between the emergency and the delivery. In many Florida birth injury cases, the limitations period generally extends until around the child’s eighth birthday, though specific deadlines can depend on the facts and statutes in effect. The delivery records must be secured before the hospital’s retention period expires.
On This Page
The Forensic Timeline: Three Windows Where Negligence Occurs
The Emergency Response That Should Have Happened and How We Prove It Did Not
The Defendants You May Not Know About
THE FORENSIC TIMELINE: THREE WINDOWS WHERE NEGLIGENCE OCCURS
Every competitor website will tell you that cord prolapse is dangerous. They will list the risk factors. They will say “call us.” None of that helps you understand whether your medical team failed. To answer that question, we reconstruct the timeline from the medical record and examine three windows where the standard of care required specific actions.
Window 1: Before the Prolapse. The Warning Signs That Were Present and Ignored.
Cord prolapse does not come out of nowhere. Certain conditions make it predictable: breech or transverse presentation, polyhydramnios (excess amniotic fluid), an unengaged fetal head at the time of membrane rupture, a long umbilical cord, or a second twin after the first has been delivered. These are documented in the prenatal record. If the mother presented to the Miami hospital with one or more of these risk factors, the obstetric team had an obligation to anticipate the possibility of prolapse and plan accordingly. That means having the operating room available, the anesthesiologist on standby, and the delivery team briefed on the need for rapid response. If the risk factors were present in the chart and the team was not prepared, the negligence began before the cord ever moved.
Window 2: The Moment of Prolapse. What the Fetal Monitor Was Showing and Whether Anyone Was Watching.
When the cord is compressed between the baby and the birth canal, the fetal heart rate tracing changes immediately. Variable decelerations, the jagged, sudden drops in heart rate that correlate with cord compression, appear on the monitor strip. In a frank prolapse, where the cord is palpable in the vaginal canal, the heart rate may drop to the 60s or 70s and stay there. This is a bradycardia that demands immediate action.
The question we ask is not whether the heart rate dropped. The question is how long it took for someone to notice, how long it took for that person to escalate to the attending physician, and how long it took for the attending to make the decision to proceed to cesarean delivery. Every minute of that chain is timestamped in the nursing notes and the electronic fetal monitoring record. If the nurse was monitoring two patients simultaneously and missed the deceleration for eight minutes, those eight minutes belong to the hospital that assigned a single nurse to two laboring patients.
Window 3: The Decision to Incision. The Minutes That Determine Whether Your Child Has a Brain Injury.
Once the decision is made to deliver by emergency cesarean, the clock starts. In obstetric training, the benchmark is 30 minutes from decision to incision for a Category I (emergent) cesarean. For cord prolapse with sustained bradycardia, many maternal-fetal medicine experts will testify that the acceptable window is closer to 10 to 15 minutes. The time it takes to transport the mother to the operating room, administer anesthesia, prep the surgical field, and begin the incision is recorded in the anesthesia record and the operative report.
In Miami birth injury litigation, we compare the decision to incision time against what the clinical urgency demanded. If the operating room was occupied and the mother waited in the hallway. If the anesthesiologist was handling another case and took 20 minutes to arrive. If the physician attempted a prolonged manual elevation of the presenting part instead of moving immediately to surgery. Each of these delays is documented. Each one is attributable to a specific defendant. And each one can be correlated by our experts with the duration of fetal oxygen deprivation that produced the injury visible on the child’s MRI.
THE EMERGENCY RESPONSE THAT SHOULD HAVE HAPPENED AND HOW WE PROVE IT DID NOT
When a cord prolapse is identified, the standard of care requires a specific sequence of immediate interventions. The provider performing the vaginal examination must keep their hand inside the birth canal and manually elevate the presenting part (the baby’s head or buttocks) off the compressed cord to restore blood flow. The mother should be repositioned into the Trendelenburg position (head down, hips elevated) or the knee-chest position to use gravity to relieve pressure on the cord. Tocolytic agents may be administered to halt contractions that are compressing the cord further. And the operating room must be activated for emergency delivery.
These are not judgment calls. They are protocols. Every obstetric resident trained in Miami-Dade County learns them. Every labor and delivery nurse is trained to execute them. The medical record tells us whether each step was performed and at what time. If the manual elevation was not maintained. If the Trendelenburg position was not initiated. If tocolytics were not considered. If the emergency cesarean was not called. Each omission narrows the defense’s ability to argue that the team responded appropriately, because the textbook response is written down, it is taught in every residency program, and the documentation either confirms compliance or exposes the gap.
THE DEFENDANTS YOU MAY NOT KNOW ABOUT
Most families assume the obstetrician is the only defendant. In cord prolapse cases, the chain of failure often extends well beyond the delivering physician.
The labor and delivery nurse is responsible for continuous fetal monitoring interpretation. If the variable decelerations or bradycardia appeared on the tracing and the nurse did not escalate to the physician within the expected timeframe, the nurse and the nursing supervisor carry individual exposure. The electronic monitoring system timestamps every alarm and every acknowledgment. We obtain those logs.
The hospital as an institution is responsible for staffing. If the operating room was not available because it was occupied by an elective procedure. If the anesthesiologist was not in the building and had to be called from home. If the labor and delivery unit was running with insufficient nurse to patient ratios. These are institutional failures, not individual ones, and the corporate entity that made the staffing and scheduling decisions is the proper defendant.
The anesthesiologist controls the second largest segment of the decision to incision timeline. If general anesthesia was required because no epidural was in place, and the anesthesiologist took longer than the urgency demanded to intubate and clear the patient for surgery, that individual’s response time is documented in the anesthesia record and becomes a separate element of the case.
WHAT COMPENSATION COVERS WHEN THE INJURY IS PERMANENT
A cord prolapse brain injury case is not about recovering the cost of the hospital bill. It is about funding every year of a life that has been permanently altered. The Life Care Plan our experts prepare projects the cost of physical therapy, occupational therapy, and speech therapy from infancy through adulthood. Adaptive equipment including wheelchairs, communication devices, and orthotics with replacement schedules tied to the child’s growth. Specialized education and individualized educational plans through the school years. Home modifications for accessibility. Modified transportation. Attendant care ranging from part-time support to around the clock nursing depending on the severity of the hypoxic injury.
A vocational economist calculates the income the child would have earned across a working lifetime absent the injury. These economic projections, combined with the Life Care Plan and adjusted for inflation over a life expectancy established by our medical experts, are the foundation of the demand. This is not about a settlement number pulled from the air. It is a dollar amount derived from documented needs projected across documented years. The defense can challenge individual line items. They cannot challenge the methodology.
The Attorney Who Knows the Defense Playbook for Cord Prolapse Cases
Attorney Jorge L. Flores spent the early years of his career on the opposite side of cases like this. As an attorney at a leading insurance defense firm in Miami, he defended hospitals against birth injury claims, including cord prolapse cases. The defense playbook is predictable. They will argue the prolapse was “unforeseeable” even when risk factors were documented in the prenatal record. They will claim the response time was “within acceptable limits” even when the operative report shows a 40 minute decision to incision interval. They will retain an expert who testifies that the brain injury was caused by a “pre-existing condition” rather than the oxygen deprivation.
Jorge Flores sat in those defense meetings. He reviewed the fetal monitoring strips with defense experts who were hired to find any 30 second segment that looked reassuring. He drafted the motions designed to exclude the plaintiff’s timeline reconstruction from evidence. That experience is now the lens through which every cord prolapse case at this firm is prepared. We anticipate the defense before they file their answer because the attorney building your case used to build theirs.
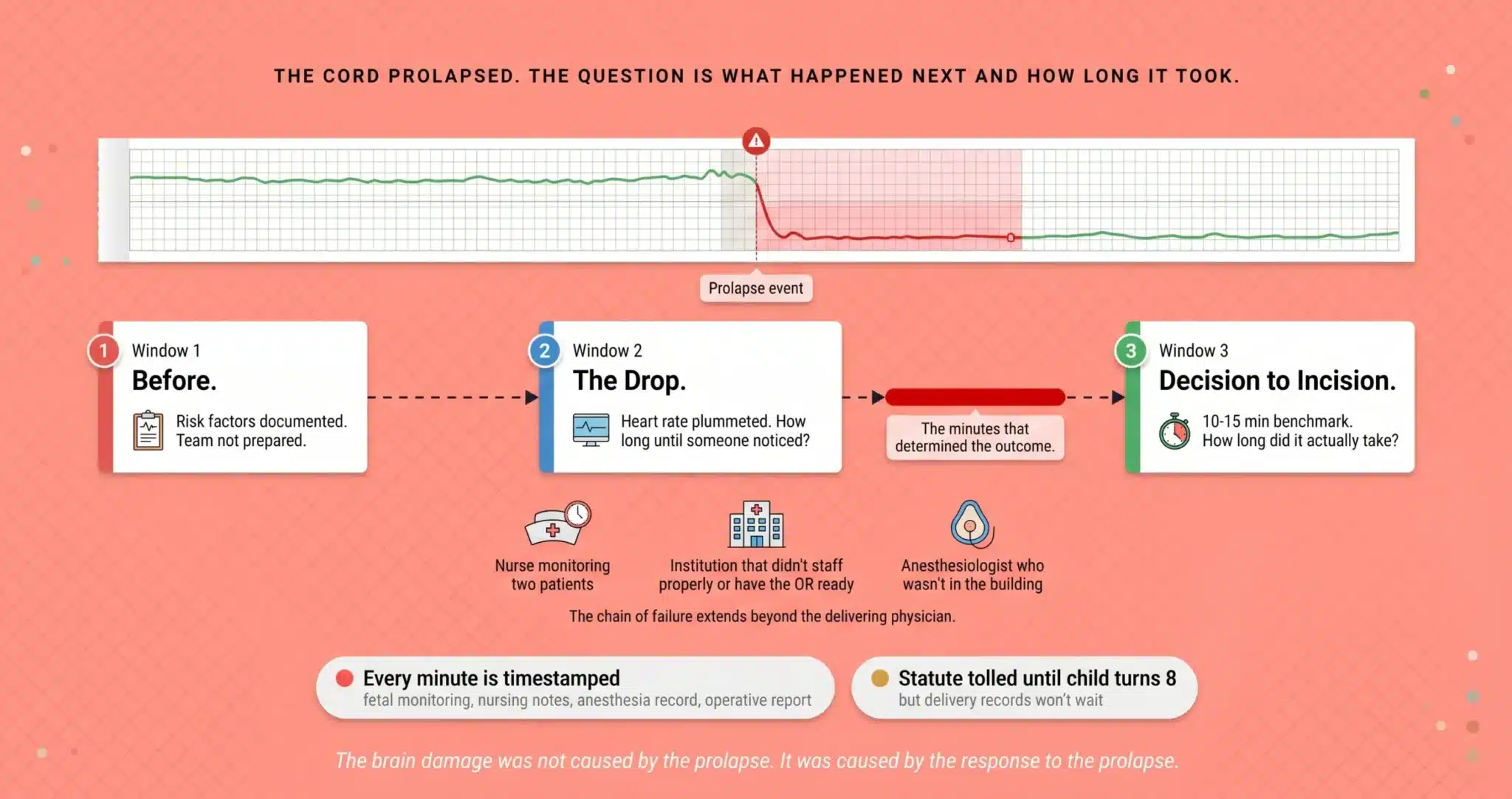
The Cord Prolapsed. The Question Is What Happened Next and How Long It Took.
The fetal monitoring strip, the nursing notes, the anesthesia record, and the operative report reconstruct the timeline minute by minute. If the minutes were lost, the timestamps do not lie.
(305) 598-2221
FREQUENTLY ASKED QUESTIONS
Is it my fault because I chose a vaginal delivery?+
No. The decision to attempt vaginal delivery is made in consultation with the obstetric team, and the physician has an obligation to advise you of the risks based on your specific pregnancy. If risk factors for cord prolapse were present and the physician did not recommend a planned cesarean or did not ensure the team was prepared for emergency delivery, the failure belongs to the medical team. You relied on their expertise. That is what it is there for.
What are “variable decelerations” and why do they matter?+
Variable decelerations are sudden drops in the fetal heart rate that appear on the electronic fetal monitoring strip. They are the signature pattern of cord compression. When they are repetitive, deep, or slow to recover, they indicate that the baby’s oxygen supply is being interrupted. In a cord prolapse, these decelerations may escalate to sustained bradycardia (heart rate below 110 for more than 10 minutes). The monitoring strip captures every one, and our maternal-fetal medicine experts analyze the pattern to determine when the clinical team should have acted.
How fast should the baby have been delivered after the cord prolapsed?+
The traditional benchmark for a Category I (emergent) cesarean is 30 minutes from decision to incision. For cord prolapse with sustained bradycardia, many experts in Miami birth injury litigation testify that the window should be 10 to 15 minutes. The operative report and the anesthesia record document the exact interval. If the team exceeded the timeframe that the clinical urgency demanded, the excess minutes are directly correlated with the duration of fetal oxygen deprivation.
Can I sue the hospital and not just the doctor?+
Yes. The hospital is responsible for staffing, equipment availability, and operational readiness. If the operating room was occupied, if the anesthesiologist was not in the building, or if the nurse to patient ratio was insufficient to maintain continuous fetal monitoring, those are institutional failures. The hospital, the attending physician, the anesthesiologist, and the nursing staff may all be named as defendants depending on where the timeline broke down.
How long do I have to file a cord prolapse injury case in Miami?+
In many Florida birth injury cases, the limitations period does not begin to run until around the child’s eighth birthday, though specific deadlines can depend on the facts and statutes in effect at the time of the injury. But the delivery room records, the electronic fetal monitoring data, the anesthesia logs, and the operative notes are stored on the hospital’s schedule, not yours. Once the retention period lapses, those files can be purged. We send statutory preservation demands the day we are retained to lock down every document before that window closes.
What does it cost to hire you for a cord prolapse birth injury case?+
There is no upfront cost and no hourly bill. We finance the entire case ourselves, from the medical records through the expert consultations, the fetal monitoring analysis, and the Life Care Plan. We collect a percentage only if we recover compensation for your family. If the case does not result in a recovery, our investment is our loss, not yours.
CONTACT US FOR A FREE CASE REVIEW
If your child suffered a brain injury following an umbilical cord prolapse at a Miami hospital and you believe the medical team’s response was delayed, the Law Offices of Jorge L. Flores, P.A., will review the delivery records at no cost. We reconstruct the timeline, identify where the response broke down, and tell you whether the evidence supports a claim.
Free Case Review. No Fee Unless We Recover Compensation.
We fund the investigation, the experts, and the Life Care Plan. There is no fee unless we recover compensation for your family.
(305) 598-2221
Related: Birth Injuries · Brain & Spinal Cord Injuries · Periventricular Leukomalacia (PVL) · Kernicterus · Medical Malpractice