

Former hospital defense attorney · Law Offices of Jorge L. Flores, P.A. · Miami, Florida
Last Updated: April 2026
Kernicterus Is Classified as a “Never Event” in Modern Medicine. If Your Child Has It, a Safety System Failed.
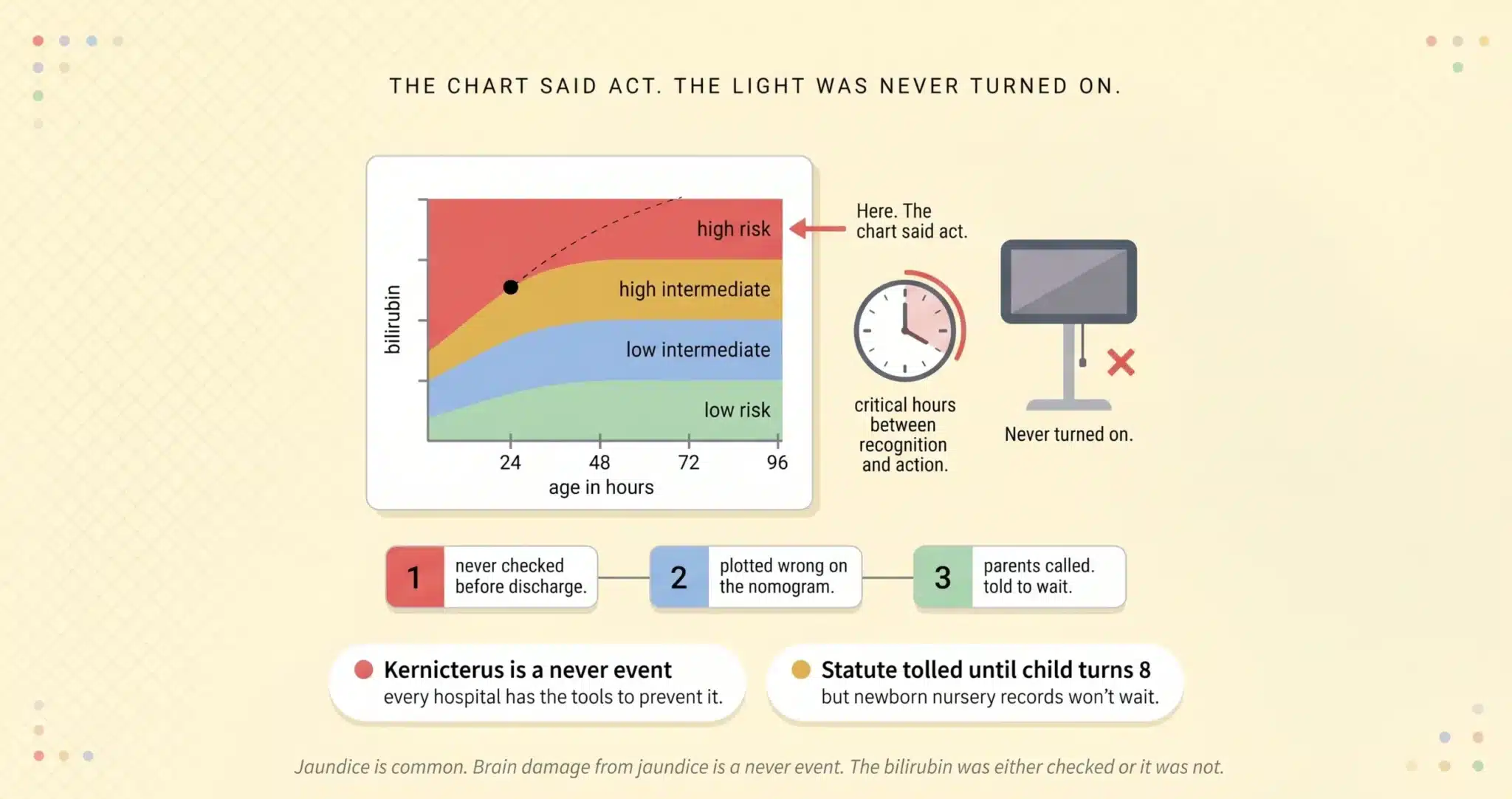
Kernicterus is not a disease. It is a permanent brain injury caused by bilirubin that was allowed to reach toxic levels in a newborn’s blood. Every hospital in Miami has the tools to prevent it. A transcutaneous bilirubin meter takes seconds to use. The Bhutani nomogram plots the result against the infant’s age in hours and tells the physician whether the level is low risk, intermediate, or in the high risk zone requiring immediate intervention. Phototherapy is available in every newborn nursery in the country. Exchange transfusion exists for the cases where phototherapy fails. The entire pathway from screening to treatment is mapped, published by the American Academy of Pediatrics, and taught in every medical school and residency program.
Kernicterus happens when that pathway is not followed. When the bilirubin is not checked before discharge. When the number is plotted incorrectly on the nomogram. When the infant is sent home at 20 hours of age without a follow up appointment. When the parents call the pediatrician to report that the baby is lethargic and feeding poorly and are told to “wait and see.” By the time the baby arrives back at the emergency room with arching, high pitched crying, and a bilirubin above 30, the damage to the basal ganglia and auditory pathways is already done.
⚠ Jaundice Is Common. Brain Damage Is Not.
If your newborn was discharged from a Miami hospital and later diagnosed with kernicterus or acute bilirubin encephalopathy, the medical team may have failed to follow the AAP screening guidelines that exist to prevent this exact injury. The filing window under Florida law generally extends until around the child’s eighth birthday for injuries to a minor, though specific deadlines can depend on the facts and statutes in effect. Hospital records must be preserved immediately.
Free Case Review: Should This Have Been Prevented? (305) 598-2221
On This Page
The Three Points Where the Safety System Breaks Down
The Bhutani Nomogram: The Chart That Proves the Hospital Knew
Basal Ganglia Damage, Auditory Neuropathy, and the Lifetime Consequences of Kernicterus
Securing Your Child’s Future: What the Life Care Plan Includes
THE THREE POINTS WHERE THE SAFETY SYSTEM BREAKS DOWN
Other law firm websites will list generic errors: “failure to diagnose,” “delayed treatment,” “medical negligence.” Those descriptions could apply to any condition. Kernicterus is different. The pathway to brain damage follows a specific, documentable sequence of failures, and the medical record captures each one in real time. These are the three breakpoints we trace in every case.
Breakpoint 1: The Bilirubin Was Never Checked Before Discharge
The AAP Clinical Practice Guideline on the management of hyperbilirubinemia in newborns 35 weeks and above (as published by the American Academy of Pediatrics and endorsed as the national standard for neonatal jaundice management) recommends universal bilirubin screening before hospital discharge. A transcutaneous bilirubinometer pressed against the infant’s sternum gives a reading in seconds. That reading, plotted against the infant’s age in hours on the Bhutani nomogram, tells the physician whether the baby is safe to go home or whether the trajectory is headed toward a dangerous zone. In the kernicterus cases we handle across Miami-Dade County, the first failure is often the simplest: the test was never performed. The baby was born, appeared healthy, and was discharged at 18 or 24 hours of age without a bilirubin level ever being drawn. The discharge summary will say “infant tolerating feeds, no jaundice noted.” Two days later, the baby is back in the ER with a total serum bilirubin above 25 mg/dL and signs of acute bilirubin encephalopathy. The hospital’s own discharge protocol required the test. The chart proves it was not done.
Breakpoint 2: The Number Was Plotted Wrong or Ignored on the Nomogram
Sometimes the bilirubin is checked. The number comes back. And then nothing happens. A total serum bilirubin of 14 mg/dL at 24 hours of life plots into the high intermediate risk zone on the Bhutani nomogram. That zone requires a repeat bilirubin within 8 to 12 hours and close follow up after discharge. But if the physician reads the number in isolation without plotting it against the infant’s age in hours, 14 may look reassuring. “Normal” bilirubin in the first days of life depends entirely on the clock. A level that is safe at 72 hours is dangerous at 24 hours because the trajectory matters more than the snapshot. The nomogram exists to force the physician to consider the trajectory. When the nomogram is not used, or when the number is plotted incorrectly, the infant is discharged into a rising bilirubin curve without the safety net that should have caught it.
Breakpoint 3: The Parents Called. They Were Told to Wait.
This is the failure that haunts the families we represent. The baby is home. The skin looks yellow. The baby is not latching. The baby sleeps through feedings and is difficult to wake. The parents call the pediatrician’s office or the hospital nursery and describe these symptoms. They are told the baby is “just sleepy,” that jaundice is “very common in newborns,” that they should try again at the next feeding and come in for a weight check in a few days.
What the parents do not know is that the symptoms they described, lethargy, poor feeding, difficulty arousing, are the clinical hallmarks of acute bilirubin encephalopathy. They are not signs of a sleepy baby. They are signs that bilirubin is crossing the blood-brain barrier and depositing in the basal ganglia and brainstem nuclei. By the time the family returns to the hospital and the total serum bilirubin comes back above 30 mg/dL, the window for effective phototherapy may have closed. Emergency exchange transfusion may or may not reverse the damage already done. The phone log, the triage notes, and the after-hours call record document exactly what the parents reported and exactly what the medical team told them to do. That record is the backbone of the case.
THE BHUTANI NOMOGRAM: THE CHART THAT PROVES THE HOSPITAL KNEW
The Bhutani nomogram is the single most important piece of evidence in a kernicterus case. Published in 1999 by Dr. Vinod Bhutani and adopted into the AAP guidelines, this hour-specific bilirubin nomogram divides newborns into four risk zones based on two data points: the total serum bilirubin level and the infant’s age in hours at the time of the measurement. A bilirubin of 12 mg/dL at 18 hours of life falls into the high risk zone. The same bilirubin at 72 hours falls into the low intermediate zone. The clinical response required by each zone is different. The high risk zone demands repeat testing in hours and consideration of immediate phototherapy. The low intermediate zone permits discharge with routine follow up.
In Miami birth injury litigation, our neonatology experts take the bilirubin values documented in the hospital record, plot each one on the nomogram at the exact hour of life it was drawn, and reconstruct the trajectory the medical team should have seen. If the infant’s bilirubin was crossing from intermediate into high risk and the team did not escalate treatment, we can demonstrate with mathematical precision the hour at which the intervention should have occurred and the hour at which it actually did. The gap between those two points is where the brain damage happened. The defense cannot argue that the nomogram does not apply. It is the national standard. It was available on every computer in that hospital. The question is whether anyone opened it.
BASAL GANGLIA DAMAGE, AUDITORY NEUROPATHY, AND THE LIFETIME CONSEQUENCES OF KERNICTERUS
Bilirubin is neurotoxic at high concentrations. It has a specific affinity for the globus pallidus and subthalamic nuclei within the basal ganglia, and for the auditory nuclei in the brainstem. The pattern of injury it produces is distinct from the white matter damage seen in PVL and from the cortical damage seen in hypoxic ischemic encephalopathy. Kernicterus leaves a signature on the MRI that a pediatric neuroradiologist can identify, and the clinical presentation that follows is equally specific.
Athetoid (dyskinetic) cerebral palsy is the form of CP most closely associated with kernicterus. Unlike the spastic diplegia that follows PVL, athetoid CP produces involuntary writhing movements, fluctuating muscle tone, and difficulty maintaining posture. The child may have normal or near-normal intelligence trapped inside a body that will not cooperate. This distinction matters for damages because a child with athetoid CP often understands their limitations fully, which compounds the non-economic impact of the injury.
Auditory neuropathy spectrum disorder (ANSD) is the second hallmark. Bilirubin damages the auditory nerve pathways, producing a form of hearing loss that is different from the sensorineural loss caused by other conditions. The cochlea may function normally while the nerve transmission to the brain is disrupted. Standard hearing aids often do not help. Cochlear implants may be indicated, but outcomes vary. Speech development is delayed or absent, and the cost of auditory rehabilitation, speech therapy, and communication technology extends across the child’s entire life.
Dental enamel dysplasia, upward gaze palsy, and cognitive processing deficits round out the kernicterus phenotype. The dental enamel abnormalities result from bilirubin deposition during tooth development. The gaze palsy reflects damage to the brainstem oculomotor pathways. The cognitive deficits may be subtle or significant depending on the extent of the bilirubin exposure. Each of these findings, documented in the child’s medical and dental records, corroborates the MRI pattern and strengthens the causal link between the untreated hyperbilirubinemia and the lifelong injury.
SECURING YOUR CHILD’S FUTURE: WHAT THE LIFE CARE PLAN INCLUDES
A kernicterus Life Care Plan is built around the specific constellation of deficits this injury produces. For the motor component: adaptive seating systems, gait trainers, and wheelchairs with replacement schedules projected through life expectancy, plus physical therapy and occupational therapy multiple times per week from childhood through adulthood. For the auditory component: cochlear implant evaluation, surgical implantation if indicated, device maintenance and upgrades, auditory verbal therapy, and speech-language pathology services that may be required for years. For the dental component: specialty pediatric dental care and restorative work necessitated by enamel dysplasia. For the cognitive and educational component: individualized education plans, assistive communication technology, cognitive rehabilitation, and vocational support. For the daily living component: attendant care ranging from part-time assistance to 24 hour supervision depending on severity, home modifications for accessibility, and modified vehicle for transportation. Loss of future earning capacity is calculated by a vocational economist based on what the child would have earned absent the injury. These projections are inflation adjusted and extend across the full life expectancy established by our medical experts.
The Attorney Who Knows How the Hospital Will Defend This Case
The defense in a kernicterus case follows a script that Attorney Jorge L. Flores memorized while working on the other side. Before founding this firm, he worked as an attorney for a leading insurance defense firm in Miami defending hospitals against birth injury claims. The hospital will argue that the jaundice was “physiologic” and within normal limits for the infant’s age. Their expert will testify that the bilirubin level “did not meet the threshold for phototherapy” at the time of discharge. They will blame the parents for not bringing the baby back sooner. They will argue that the infant had an “underlying hemolytic condition” that made kernicterus unavoidable regardless of the care provided.
Jorge Flores has heard every one of these arguments from the inside of the defense conference room. He knows which ones collapse under cross examination when the plaintiff’s attorney can place the bilirubin on the Bhutani nomogram at the exact hour of life and show the jury that the number was in the high risk zone before the baby ever left the hospital. The defense needs ambiguity to survive. We eliminate it.
Jaundice Is Common. Brain Damage From Jaundice Is a Never Event.
The bilirubin was either checked or it was not. The nomogram was either consulted or it was not. Phototherapy was either started or it was not. The medical record answers every one of these questions.
(305) 598-2221
FREQUENTLY ASKED QUESTIONS
My baby had jaundice but the hospital said it was normal. Could it still be malpractice?+
Jaundice is common in newborns. Kernicterus is not. The difference is whether the bilirubin level was tested, plotted on the Bhutani nomogram, and managed according to the AAP guidelines. If the hospital called the jaundice “normal” without checking the bilirubin, or checked it but did not plot it against the infant’s age in hours, the jaundice may have been dismissed as physiologic when the trajectory was actually pathologic. The record tells us which it was.
Can kernicterus be reversed?+
No. Once bilirubin has deposited in the basal ganglia and auditory nuclei, the damage is permanent. Acute bilirubin encephalopathy can sometimes be halted with emergency exchange transfusion if caught early enough, but chronic bilirubin encephalopathy (kernicterus) represents irreversible injury. That is why the compensation in these cases must account for the full lifetime of care, equipment, therapy, and lost earning capacity the child will require.
Should I have caught the warning signs myself? Is this my fault?+
No. You are not a neonatologist. You are not trained to interpret bilirubin levels or predict trajectories on a nomogram. The responsibility to screen for hyperbilirubinemia, assess the risk zone, schedule appropriate follow up, and respond to your phone calls describing warning symptoms belongs entirely to the medical team. Parents who called their pediatrician’s office to report lethargy and poor feeding did exactly what they were supposed to do. The failure was on the other end of the phone.
What is the Bhutani nomogram and why does it matter?+
The Bhutani nomogram is a graph that plots total serum bilirubin against the infant’s age in hours. It divides newborns into four risk zones: low, low intermediate, high intermediate, and high. The zone determines the clinical response. A bilirubin of 12 at 24 hours requires a fundamentally different response than 12 at 72 hours. It is the national standard for neonatal jaundice management and is endorsed by the AAP. If the hospital did not use it, or plotted the values incorrectly, that is documentable evidence of a departure from the standard of care.
How long do I have to file a kernicterus case in Miami?+
In many Florida birth injury cases, the limitations period for a minor does not begin to run until around the child’s eighth birthday, though specific deadlines can depend on the facts and statutes in effect at the time of the injury. However, the newborn nursery records, the bilirubin lab results, the discharge risk assessment, the after-hours call logs, and the readmission labs must be preserved before the hospital’s retention period expires. We issue statutory preservation requests immediately upon engagement to protect this evidence.
What does it cost to hire you for a kernicterus case?+
You pay zero out of pocket. We fund the medical record retrieval, the neonatology expert review, the pediatric neuroradiology consultation, the audiology assessment, the Life Care Plan, and the vocational economics report ourselves. Our fee is a percentage of the recovery. If there is no recovery, there is no fee.
CONTACT US FOR A FREE CASE REVIEW
If your child has been diagnosed with kernicterus or chronic bilirubin encephalopathy following newborn jaundice at a Miami hospital, the Law Offices of Jorge L. Flores, P.A., offers a free, confidential review of the hospital records. We will plot the bilirubin values on the Bhutani nomogram, evaluate the discharge and follow up documentation, and tell you whether the evidence supports a claim.
Free Case Review. No Fee Unless We Recover Compensation.
We advance all costs of the investigation, the medical experts, and the Life Care Plan. You pay nothing unless we win.
(305) 598-2221
Related: Birth Injuries · Brain & Spinal Cord Injuries · Periventricular Leukomalacia (PVL) · Medical Malpractice