

Former hospital defense attorney · Law Offices of Jorge L. Flores, P.A. · Miami, Florida
Last Updated: April 2026
Distinguishing Between Premature Birth Risks and Preventable Medical Negligence in Miami
A diagnosis of periventricular leukomalacia often comes with an explanation that “these things happen” with premature babies. The neonatologist will point to the gestational age. The hospital discharge summary will reference the “inherent risks of prematurity.” And the parents, overwhelmed and exhausted and afraid, will accept that explanation because nobody in the room is telling them the other possibility: that the damage to their baby’s brain was not inevitable. That it was the result of specific, identifiable failures in monitoring, ventilation, or infection management that fell below the standard of care owed to every infant born in a Miami hospital.
Prematurity makes the developing brain vulnerable. That is a medical fact. But vulnerability is not the same as inevitability. The standard of care exists precisely because premature infants are fragile. When a NICU team fails to protect a brain they knew was at risk, the diagnosis is not just PVL. It is preventable PVL. And the legal question is not whether prematurity contributed. The legal question is whether the medical team did what they were required to do for a patient they knew was premature.
⚠ Was Your Child’s PVL Preventable?
Florida law gives you two years from the date you discovered the injury to file a medical malpractice claim, but the mandatory 90 day presuit investigation must be completed first. For injuries to a minor, the limitations period generally does not begin to run until around the child’s eighth birthday, though specific deadlines can vary based on the facts and statutes in effect at the time of the injury. Early investigation preserves the NICU records, ventilator logs, and fetal monitoring data that hospitals are not required to store indefinitely.
Your Child’s PVL May Have Been Preventable If:
✓ Your labor involved prolonged fetal heart rate decelerations or a Category III tracing before delivery.
✓ You had a fever, elevated white blood cell count, or other signs of infection during labor that were not treated with antibiotics before delivery.
✓ Your baby was placed on a mechanical ventilator in the NICU and blood gas results later showed CO2 levels dropped below normal range.
✓ There was a significant delay between signs of fetal distress and the decision to perform a cesarean delivery.
✓ Your child was discharged from the NICU with a “normal” prognosis but later diagnosed with cerebral palsy or developmental delays.
If any of these describe your experience, the NICU records and fetal monitoring data deserve an independent medical review. We arrange that review at no cost to your family.
On This Page
How PVL Happens: The Two Mechanisms Your Hospital Will Not Explain
The Red Flags We Look for in the Medical Records
PVL and Cerebral Palsy: The MRI Finding and the Diagnosis That Follows
HOW PVL HAPPENS: THE TWO MECHANISMS YOUR HOSPITAL WILL NOT EXPLAIN
PVL is damage to the white matter surrounding the ventricles of the brain. The white matter contains the nerve fibers that transmit signals between the brain and the body. When it is destroyed, those signals are permanently disrupted. The child may develop motor deficits, cognitive delays, or cerebral palsy depending on the extent and location of the damage. Competitors will stop the explanation here. We do not. Because the question that matters for your case is not what PVL is. It is what caused it. And in the cases we handle across Miami-Dade County and South Florida, the cause traces back to one of two mechanisms that the medical team had the ability and the obligation to prevent.
Mechanism 1: Ischemia (Loss of Blood Flow to the Brain)
The periventricular white matter in a premature infant is supplied by a fragile network of blood vessels that are exquisitely sensitive to drops in blood pressure or oxygen saturation. When blood flow to this region is interrupted or reduced, the white matter cells die. They do not regenerate. The injury is permanent. In the cases we handle, the ischemia traces back to specific clinical failures: a drop in fetal heart rate that was observed on the monitor but not acted on within the appropriate window, a neonatal blood pressure that fell below the threshold for cerebral perfusion and was not corrected in time, or a delayed cesarean delivery that left the baby in distress longer than the brain could tolerate. The fetal monitoring strips and the NICU flowsheets document every vital sign, every alarm, and every intervention in real time. Those records tell us whether the team responded or whether they waited.
Mechanism 2: Infection (Chorioamnionitis and the Inflammatory Cascade)
Chorioamnionitis is an infection of the amniotic membranes. It is diagnosed clinically when the mother develops a fever, elevated white blood cell count, uterine tenderness, or foul-smelling amniotic fluid. When chorioamnionitis is present and untreated, the inflammatory cytokines released by the infection cross the placenta and directly damage the developing white matter. This is not a subtle process. The maternal chart documents the temperature readings, the lab results, and the clinical observations in sequence. The question in every case is whether the obstetric team recognized the infection, how long they waited before initiating antibiotics or delivery, and whether the delay between recognition and action was long enough to allow the inflammatory cascade to reach the baby’s brain. In our experience, the defense will argue the infection was “subclinical” or “not yet established.” The maternal vitals and the lab trends tell a different story.
THE RED FLAGS WE LOOK FOR IN THE MEDICAL RECORDS
When a family contacts us with a PVL diagnosis from a Miami-area hospital, the first thing we request is the complete medical record from the labor and delivery, the NICU admission, and the neonatal course. Our medical experts review these records for specific patterns that distinguish preventable injury from unavoidable prematurity complications. These are the findings that change a case from “tragic but defensible” to “negligent and provable.”
Hypocarbia from over-ventilation. When a premature infant is placed on a mechanical ventilator in the NICU, the settings must be calibrated to the infant’s size, gestational age, and lung compliance. If the ventilator rate or tidal volume is set too aggressively, CO2 levels in the blood drop below the safe threshold. This is called hypocarbia. Low CO2 causes the cerebral blood vessels to constrict, reducing blood flow to the periventricular white matter at exactly the moment when that tissue is most vulnerable. The ventilator settings and the arterial blood gas results are recorded in the NICU flowsheet. If the CO2 dropped below 35 mmHg and the team did not adjust the ventilator settings promptly, we have a documented window of preventable ischemia.
Delayed cesarean delivery. The electronic fetal monitoring strips show the baby’s heart rate pattern throughout labor. Category III tracings, absent variability with recurrent late decelerations, nonreassuring patterns that persist without intervention, these are the signals that the baby is running out of reserve. When the obstetric team observes these patterns and does not move to an emergency cesarean within the timeframe the clinical situation demanded, the minutes that pass between recognition and delivery are the minutes during which the white matter is being destroyed. We retain maternal-fetal medicine specialists who re-read the strips and calculate whether the response time met or fell short of what the clinical picture required.
Untreated maternal infection. Group B Streptococcus (GBS) screening, maternal temperature trending upward, an elevated white blood cell count, foul-smelling amniotic fluid after rupture of membranes. These are the clinical markers of chorioamnionitis that the obstetric team is trained to recognize and act upon. When the markers were documented in the chart and the team delayed antibiotic administration or continued to manage labor instead of expediting delivery, the interval between the first clinical sign and the first intervention is the interval we present to the jury.
Mismanaged neonatal resuscitation. The first minutes after delivery of a premature infant are the most consequential of that child’s life. The resuscitation must follow the Neonatal Resuscitation Program (NRP) guidelines: controlled ventilation, appropriate oxygen titration, avoidance of excessive positive pressure that can cause lung injury and subsequent hemodynamic instability. An overly aggressive resuscitation, one that hyperventilates the infant and drives CO2 too low, can initiate the same ischemic cascade that causes PVL. The delivery room notes and the initial NICU admission vitals tell us whether the resuscitation was measured or whether it was reactive.
PVL AND CEREBRAL PALSY: THE MRI FINDING AND THE DIAGNOSIS THAT FOLLOWS
PVL is what the MRI shows. Cerebral palsy is what the neurologist diagnoses when the child begins missing developmental milestones. They are not the same thing, but they are connected in the majority of cases we handle. The white matter damage visible on the MRI disrupts the motor pathways that control movement. As the child grows, the effects of that disruption become apparent: delayed walking, spasticity in the legs (spastic diplegia is the most common pattern with PVL), difficulty with fine motor skills, and in more severe cases, involvement of all four limbs.
The defense will argue that cerebral palsy has “many causes” and that PVL is “commonly seen in premature infants regardless of care.” That argument works when the plaintiff’s attorney allows the conversation to remain abstract. It fails when the plaintiff’s attorney presents the specific ventilator settings, the specific blood gas results, the specific fetal monitoring patterns, and the specific timeline of the infection alongside the MRI showing the exact anatomical location of the white matter destruction. In Miami birth injury litigation, we retain pediatric neuroradiologists who correlate the MRI findings with the clinical timeline to demonstrate that the pattern of injury is consistent with the specific mechanism of negligence documented in the chart.
WHAT A LIFE CARE PLAN COVERS FOR A CHILD WITH PVL
The value of a PVL case is not measured by the hospital bill from the NICU stay. It is measured by the cost of living with the injury for the rest of the child’s life. For families in Miami and throughout South Florida, we retain Life Care Planners and Vocational Economists who build a projection based on the child’s specific diagnosis, the severity of the motor and cognitive deficits, and the life expectancy established by our medical experts.
The Life Care Plan typically includes: assistive mobility equipment (wheelchair, gait trainer, stander) with replacement schedules projected through life expectancy. Physical therapy, occupational therapy, and speech therapy from childhood through adulthood, with frequency adjustments as the child’s needs evolve. Orthopedic interventions including bracing, Botox injections for spasticity management, and potential surgical procedures such as selective dorsal rhizotomy or tendon lengthening. Home modifications for wheelchair accessibility including ramps, widened doorways, accessible bathrooms, and adaptive kitchen equipment. Modified vehicle for transportation. Special education support, tutoring, and cognitive rehabilitation. Loss of future earning capacity based on the vocational economist’s projection of what the child would have earned absent the injury. And 24 hour attendant care if the severity of the motor deficits requires it. These projections routinely produce seven and eight figure calculations that a defense team cannot dismiss with a two page IME report.
Why the Attorney Who Handles Your PVL Case Matters
The hospital’s defense in a PVL case is predictable because Attorney Jorge L. Flores spent years helping build it. Before founding this firm, he worked as an attorney for a leading insurance defense firm in Miami, where he defended hospitals and their insurers against birth injury claims. He sat in the rooms where defense neonatologists rehearsed testimony explaining that PVL is “a known consequence of prematurity.” He reviewed the NICU records alongside defense experts who were hired to find language in the chart that would shift causation away from the medical team and toward the infant’s gestational age. He knows that the defense’s first move in every PVL case is to make prematurity the villain and the hospital the bystander. That framing collapses when the plaintiff’s attorney can point to the specific ventilator setting that drove CO2 below 35, the specific hour when the maternal temperature spiked and antibiotics were not started, or the specific fetal monitoring strip that showed Category III tracings 40 minutes before the cesarean was called. Jorge Flores knows what the defense needs to win. He builds the case to take it away from them.
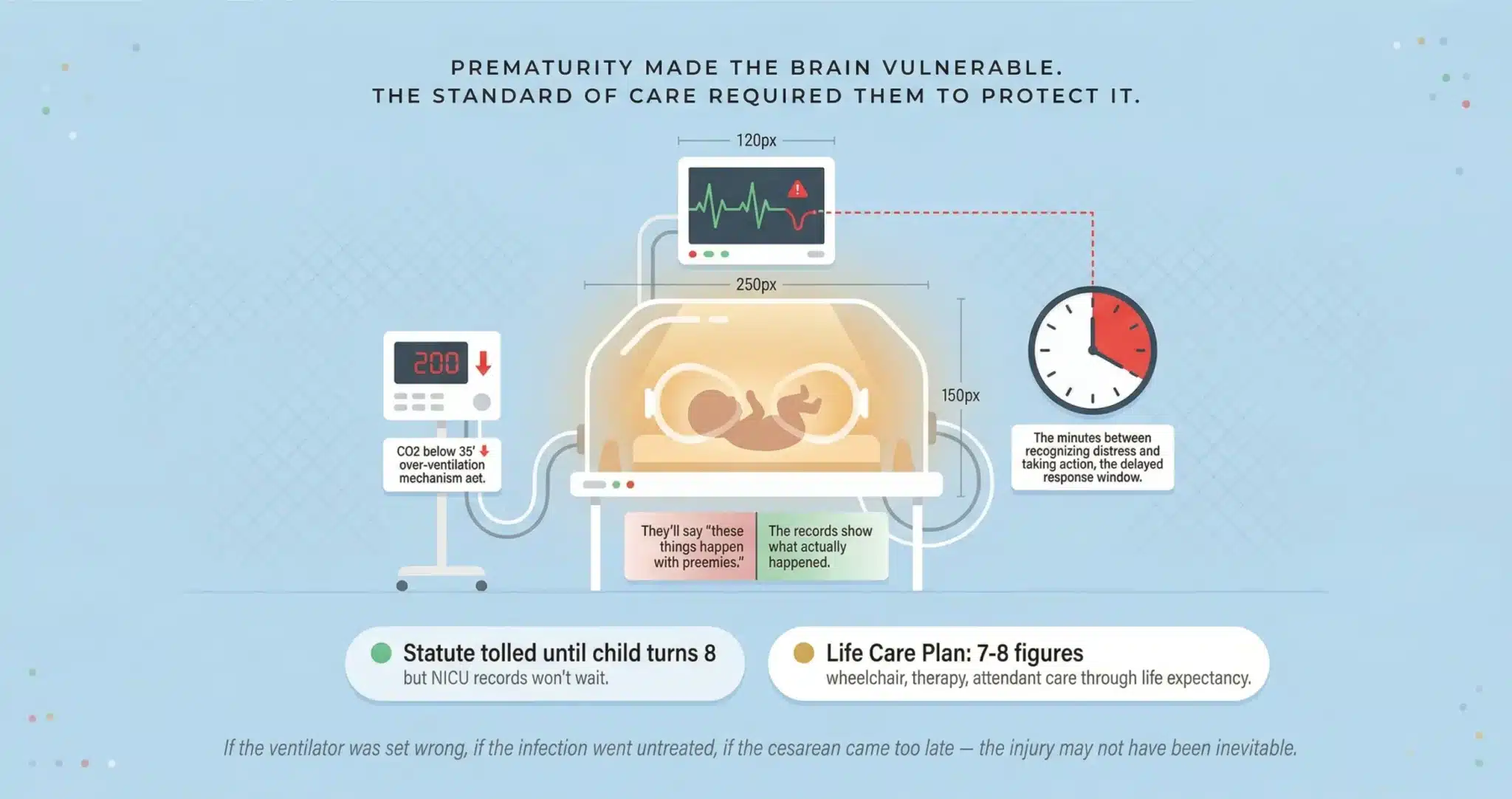
Prematurity Made the Brain Vulnerable. The Standard of Care Required the Medical Team to Protect It.
If the ventilator settings were wrong, if the infection went untreated, if the cesarean came too late, your child’s PVL may not have been inevitable. We review the records and tell you what happened.
(305) 598-2221
FREQUENTLY ASKED QUESTIONS
My baby was born at 28 weeks. Is PVL just normal for preemies?+
Prematurity makes the periventricular white matter vulnerable, but the standard of care exists specifically to protect vulnerable brains. NICU protocols for ventilator management, blood pressure maintenance, and infection control are designed for premature infants. If the medical team failed to follow those protocols, the prematurity does not excuse the negligence. It makes the negligence more consequential.
What is hypocarbia and how does it cause PVL?+
Hypocarbia is abnormally low carbon dioxide in the blood, typically caused by ventilator settings that are too aggressive for the infant’s size and lung compliance. When CO2 drops below approximately 35 mmHg, the cerebral blood vessels constrict, reducing blood flow to the periventricular white matter. If the NICU team did not monitor arterial blood gases frequently enough or did not adjust ventilator settings when the CO2 trended downward, the resulting ischemia can destroy the white matter and cause PVL.
Does PVL always lead to cerebral palsy?+
Not always, but frequently. The white matter damaged in PVL contains the motor pathways that control movement. Many children with PVL develop spastic diplegia, a form of cerebral palsy that primarily affects the legs. The severity depends on the extent and location of the white matter injury. Milder PVL may produce subtle motor delays or learning disabilities. Severe PVL can result in quadriplegia. The MRI findings, correlated with the clinical presentation, determine the projected lifetime impact that forms the basis of the Life Care Plan.
How long do I have to file a PVL birth injury case in Miami?+
In many Florida birth injury cases, the limitations period for a minor does not begin to run until around the child’s eighth birthday, but specific deadlines can vary based on the facts and the statutes in effect at the time of the injury. However, the NICU ventilator logs, arterial blood gas records, fetal monitoring strips, and nursing flowsheets must be secured before the hospital’s internal retention period expires. Hospitals are not required to preserve these records indefinitely. We recommend contacting us as early as possible so we can issue statutory preservation requests before critical evidence is destroyed.
What is a Life Care Plan and why does it matter in a PVL case?+
A Life Care Plan is a document prepared by a certified Life Care Planner that projects the cost of every medical service, piece of equipment, therapy, educational support, home modification, and attendant care the child will need from the date of the injury through their life expectancy. It transforms abstract “pain and suffering” into a concrete, itemized, inflation-adjusted calculation that a jury can act on. Without a Life Care Plan, the defense will argue the child is “doing fine” based on a single afternoon examination. With one, the jury sees the full cost of what was taken.
What does it cost to hire you for a PVL birth injury case?+
You pay zero out of pocket. We fund the medical record retrieval, the expert review of the NICU records and fetal monitoring strips, the neuroradiology consultation, the Life Care Plan, and the vocational economics report ourselves. Our fee comes from the recovery. If there is no recovery, there is no fee.
CONTACT US FOR A FREE CASE REVIEW
If your child has been diagnosed with periventricular leukomalacia at a Miami hospital and you believe the injury may have been preventable, the Law Offices of Jorge L. Flores, P.A., offers a free, confidential review of your medical records. We will tell you whether the evidence supports a claim and explain exactly what a case would involve.
Free Case Review. No Fee Unless We Recover Compensation.
We advance all costs of the investigation, the medical experts, and the Life Care Plan. You pay nothing unless we win.
(305) 598-2221
Related: Birth Injuries · Brain & Spinal Cord Injuries · Medical Malpractice · Wrongful Death